



Abstract
Cerebral amyloid angiopathy-related inflammation (CAA-ri) is a rare but treatable CAA subtype characterized by reversible inflammatory mechanisms, offering unique diagnostic and therapeutic potential. We report a CAA-ri case featuring left-dominant cerebral microbleeds (baseline: 38 left vs. 2 right; 13-month progression to 65 left) with rapid clinical improvement post-corticosteroid therapy. This case expands the phenotypic spectrum of CAA-ri by demonstrating asymmetric CMBs with unilateral progression—a previously underrecognized pattern. This presentation requires heightened awareness in clinical practice to avert misdiagnosis and overlooked diagnoses.
Keywords:Cerebral Amyloid Angiopathy-Related Inflammation; Unilateral Cerebral Microbleeds.
Introduction
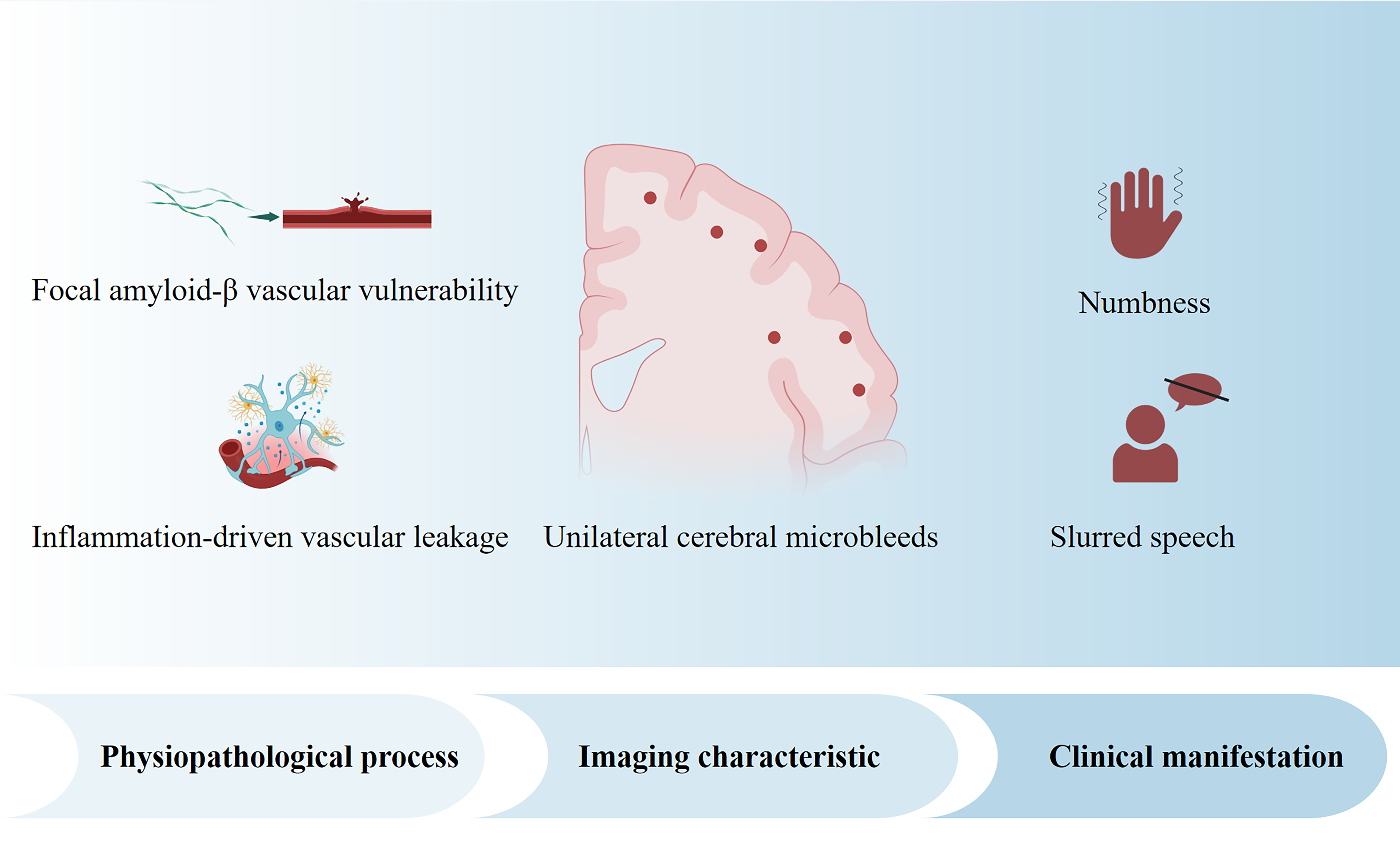
Cerebral amyloid angiopathy-related inflammation (CAA-ri) is defined as a pathological condition characterized by perivascular and intravascular inflammation, which is triggered by the deposition of vascular amyloid-beta (Aβ), leading to local blood-brain barrier leakage and culminating in vascular rupture. Common features of CAA-ri are rapid progressive dementia, epileptic seizures, headaches, and MRI findings showing single or multiple focal white matter hyperintensities on T2-weighted sequences and cortical microbleeds[1]. It is important to note that in the case of CAA-ri, the CMB distribution pattern is predominantly bilateral and asymmetric[2]. No cases of CAA-ri with strictly unilateral progress have been reported to date. So recognizing the rare clinical manifestations of CAA-ri is of great significance. Since its treatment differs significantly from that of typical CAA, and CAA-ri exhibits a favorable response to immunosuppressive therapy.
Here, we report a case of CAA-ri with strict unilateral rapid progressive CMB as the main manifestation and the chief complaint was recurrent and transient numbness in the right limbs. The patient's condition was successfully managed with methylprednisolone pulse therapy.
Case Presentation
A 60-year-old male patient presented to our hospital multiple times within 15 months due to recurrent episodes of slurred speech and right limb numbness. Each episode lasted 5-8 minutes and resolved completely without residual symptoms. Head susceptibility-weighted imaging (SWI) revealed multiple cerebral microbleeds (CMBs) in the left hemisphere. There was no relevant family history(e.g. cerebrovascular disease, dementia, and hereditary small vessel disease).
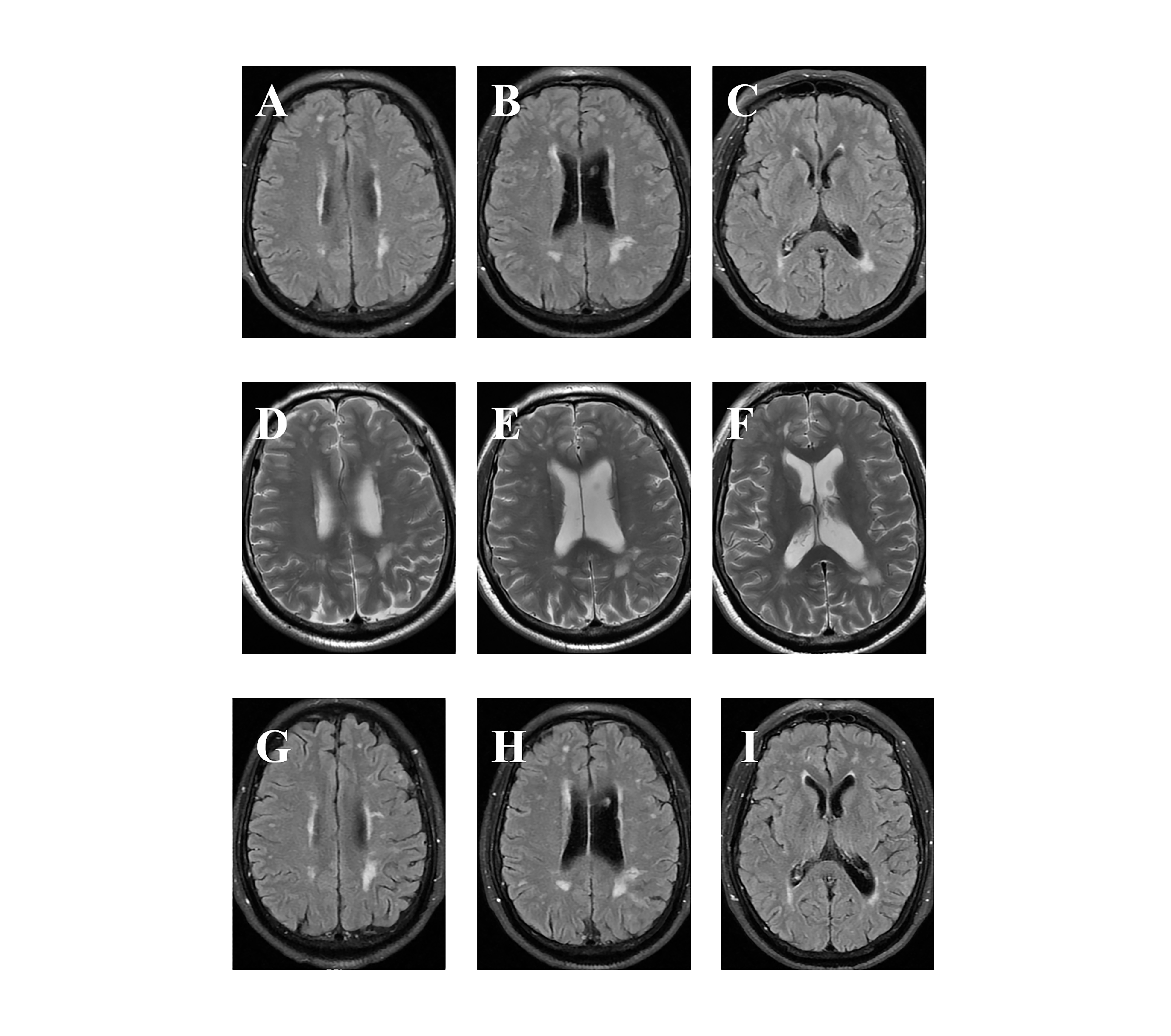
The patient first sought medical attention in November 2023 due to "Recurrent numbness in the right limbs and slurred speech for 3 months". Magnetic resonance imaging (MRI) with T1, T2, and SWI sequences showed multiple microbleeds in the left cerebral hemisphere (frontal, parietal, occipital and temporal lobe), periventricular white matter hyperintensity (Fazekas grade II), and scattered lacunar lesions in the lateral ventricles and semioval center. To evaluate venous drainage abnormalities, MR venography (MRV) showed superior drainage in the left transverse sinus and sigmoid sinus, with local stenosis in the distal ends of both transverse sinuses. To confirm venous stenosis and exclude arteriovenous malformation, digital subtraction angiography (DSA) was performed, and the results were bilateral transverse sinus stenosis (left > right), no evidence of shunting or vascular malformations. The patient's follow-up head MRI during the 12-month follow-up showed a progressive increase in microbleeds (from 38 to 65 lesions) within the left hemisphere, suggesting ongoing vascular pathology (Figure 1 A-F). However, no significant progression of WMH (white matter hyperintensity) lesions was observed (Figure 2 A-F). To exclude infectious, inflammatory, or neurodegenerative etiologies, cerebrospinal fluid (CSF) analysis including GFAP and Alzheimer's disease (AD) biomarkers was performed and the results showed pathological manifestations related to AD (Number of nucleated cells: 1 x 10 ^ 6/L, GFAP: 8.44 pg/mL [normal≤30], Aβ42: 140.15pg/mL [normal>609.4 pg/mL], Aβ42/Aβ40: 0.024pg/mL [normal>0.055]). Moreover, whole-exome sequencing (20858 genes) and mitochondrial genome analysis (37 genes) ruled out pathogenic variants in hereditary small-vessel disease genes (NOTCH3, COL4A1, TREX1) and mitochondrial disorders, confirming the absence of monogenic causation. According to the Criteria for the Diagnosis of CAA-ri, our case meets probable CAA - ri (Table 1)[1]. However, the attack characteristics of patients (transient, repetitive, and stereotyped episodes) align with transient focal neurological episodes (TFNE), necessitating differentiation from CAA-ri[3]. TFNE typically follows a self-limiting pattern, with symptoms improving and resolving over days to weeks. Besides, TFNE shows no improvement with corticosteroids. The patient subsequently received methylprednisolone pulse therapy and slow tapering to oral prednisone. During the follow-up after hormone therapy, the patient reported complete resolution of episodic slurred speech and no recurrence of right limbs numbness. The follow-up brain MRI (Figure 1 G-I and Figure 2 G-I) performed in April 2025 demonstrated stable cerebral microbleed burden.
Table 1. Criteria for the diagnosis of cerebral amyloid angiopathy-related inflammation (CAA-ri).
| Diagnosis | Criteria |
|---|---|
| Probable CAA-ri |
|
| Possible CAA-ri |
|
Figure 1. Longitudinal SWI demonstrating unilateral progression of cerebral microbleeds (CMBs) in the left hemisphere. (A-C) Baseline SWI (November 2023). (D-F) Follow-up SWI (December 2024).
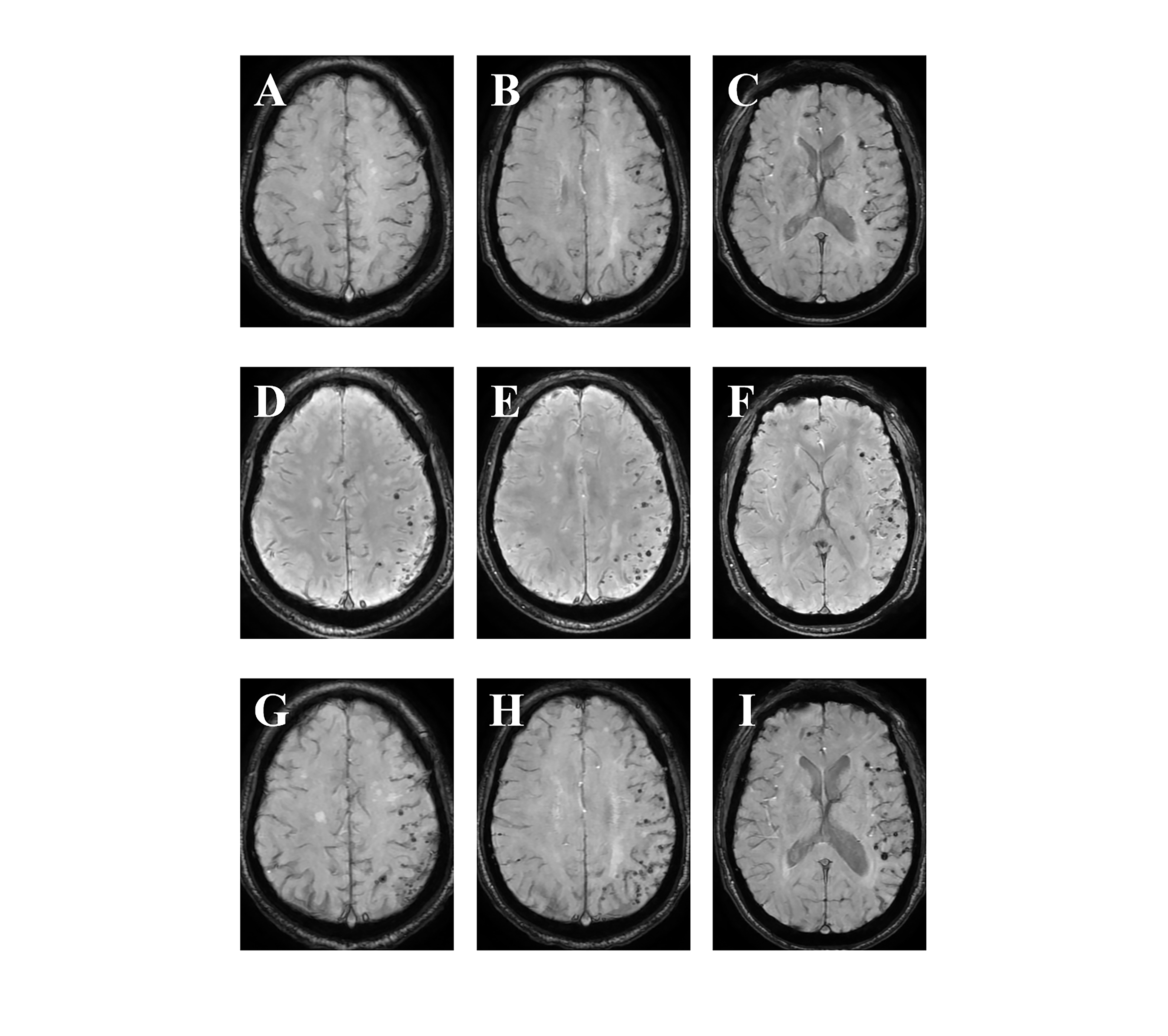
Figure 2. Longitudinal asymmetric white matter hyperintensities (WMH) on T2 imaging. (A-C) Baseline T2-FLAIR images (November 2023). (D-F) Follow-up T2-weighted images (December 2024).
Discussion
This case delineates a novel CAA-ri phenotype characterized by predominantly unilateral progression of cerebral microbleeds (CMBs) alongside definitive amyloid pathology (CSF Aβ42: 140.15 pg/mL [normal >609.4 pg/mL]; Aβ42/Aβ40: 0.024 [normal >0.055]). While classic CAA-ri exhibits bilateral lobar CMBs with vasogenic edema, the striking left hemispheric burden (38 baseline → 65 lesions) and delayed contralateral microbleeds (2 static lesions) suggest compartmentalized perivascular inflammation superimposed on diffuse amyloidosis.
CSF profiles were consistent with cerebral amyloidosis, reflecting cerebral amyloid-β deposition, these changes also characterize cerebral amyloid angiopathy (CAA) and its inflammatory subtype (CAA-ri). It typically associated with bilateral lobar CMBs in CAA and CAA-ri. However, the strictly left-sided predominance of microbleeds defies this pattern. We hypothesize two non-exclusive mechanisms: ①.Focal amyloid-β vascular vulnerability: Regional differences in vascular Aβ clearance or inflammatory activation may lead to asymmetric CMBs despite global amyloid burden. The specific distribution of the microbleeds provides evidence for a localized Aβ deposition that triggered the focal inflammatory response. Autopsy studies have shown patchy Aβ distribution in CAA[4]. ②.Inflammation-driven vascular leakage: The patient’s steroid-responsive symptoms suggest superimposed perivascular inflammation, which could exacerbate erythrocyte extravasation in amyloid-laden vessels, disproportionately affecting one hemisphere. The extensive T2/FLAIR hyperintensities, which co-localized with the cluster of progressing microbleeds, provide a radiological correlate for this localized inflammation and associated vasogenic edema[5]. Such lateralized progression may represent an early stage of CAA-ri, wherein unilateral blood brain barrier (BBB) breakdown precedes bilateral involvement. Longitudinal SWI monitoring is critical to capture this dynamic evolution.
Although brain biopsy is the diagnostic gold standard for CAA-ri, its invasive nature and risk of hemorrhagic complications limit routine clinical use. This underscores the value of recognizing distinctive clinical and imaging features, such as subacute cognitive decline, epilepsy, asymmetric white matter/cortical changes, dominant unilateral microbleeds (a less common but suggestive finding) to support non-invasive diagnosis. Immunosuppressive therapy has demonstrated efficacy in improving clinical and radiographic outcomes while reducing relapse rates in CAA-ri. After 6-month follow-up, immunosuppressive therapy effectively controlled the patient's right limb numbness.
Conclusion
In this report, we have described a unique case of CAA-ri characterized by a previously unreported pattern of strictly unilateral, rapidly progressing cerebral microbleeds. This case demonstrates that the neuroimaging spectrum of CAA-ri is broader than traditionally perceived. The key clinical implication is that the presence of such an asymmetric, progressive pattern of microbleeds should raise a high index of suspicion for the highly treatable diagnosis of CAA-ri. This awareness is critical to prevent misdiagnosis and to facilitate the timely initiation of corticosteroid therapy.
Abbreviations
Aβ: amyloid-beta; AD: Alzheimer's disease; BBB: blood brain barrier; CAA-ri: cerebral amyloid angiopathy-related inflam-mation; CMBs: cerebral microbleeds; CSF: cerebrospinal fluid; DSA: digital subtraction angiography; ICH: intracerebral hem-orrhage; MRI: magnetic resonance imaging; MRV: MR venog-raphy; SWI: susceptibility-weighted imaging; TFNE: transient focal neurological episode; WMH: white matter hyperintensity.
Declarations
Author Contributions
Lili Tang and Yujia Jin collected data and drafted the manu-script. Bingqian Wang and Yin Hu created the figures. Lusha Tong and Qiang Du revised the manuscript and conceived the study.
Acknowledgment
Not applicable.
Funding Information
None.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of The Second Affiliated Hospital of Zhejiang University School of Medi-cine (Approval Number: (2025) No. 1017).
Competing Interests
The authors declare no competing interests.
Data Availability
Not applicable.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Longitudinal SWI demonstrating unilateral progression of cerebral microbleeds (CMBs) in the left hemisphere. (A-C) Baseline SWI (November 2023). (D-F) Follow-up SWI (December 2024).
Figure 2. Longitudinal asymmetric white matter hyperintensities (WMH) on T2 imaging. (A-C) Baseline T2-FLAIR images (November 2023). (D-F) Follow-up T2-weighted images (December 2024).
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-09-13
Accepted 2025-09-21
Published 2025-10-26