



Abstract
Non-invasive brain stimulation (NIBS) modalities—including transcranial magnetic stimulation (TMS), theta-burst stimulation (TBS), and transcranial direct current stimulation (tDCS)—have emerged as promising approaches to promote language recovery in post-stroke aphasia by engaging both functional and structural neuroplasticity. This structured narrative review integrates recent multimodal evidence from functional magnetic resonance imaging (fMRI), DTI, and connectome analyses to delineate the stage-dependent mechanisms underlying NIBS-induced modulation of language networks. Findings across studies suggest a dynamic pattern of reorganization: acute-phase hypoactivation of left-hemisphere language areas and diffuse right-hemisphere disinhibition give way to bilateral upregulation in the subacute phase, followed by gradual restoration of left-dominant connectivity during the chronic stage, which may be limited by persistent contralesional hyperactivity. Low-frequency TMS or continuous TBS targeting right-hemisphere homologues can suppress maladaptive overcompensation, whereas high-frequency TMS or intermittent TBS applied to residual left-hemisphere sites enhances excitability and network centrality. Bilateral or neuronavigation-guided tDCS, particularly when combined with language training, rebalances interhemispheric excitability and supports sustained gains in naming and fluency. DTI-derived increases in arcuate and uncinate fasciculi integrity correlate with clinical improvement, while contralesional temporoparietal cortical thickening reflects concurrent structural remodeling.
Keywords:Non-invasive brain stimulation; Post-stroke aphasia; Functional magnetic resonance imaging.
Introduction
Post-stroke aphasia (PSA) is one of the most common and debilitating neurological complications following cerebrovascular accidents, with an incidence rate of approximately 30%–40%[31]. The underlying pathology primarily involves neuronal dysfunction or structural damage in the perisylvian language network of the left cerebral hemisphere—most notably in Broca’s area (Brodmann areas 44/45), Wernicke’s area (Brodmann area 22), and their subcortical connecting pathways such as the arcuate fasciculus—resulting from acute ischemic or hemorrhagic events[26]. Based on lesion location and clinical presentation, PSA can be classified into several subtypes, including expressive aphasia (Broca’s), receptive aphasia (Wernicke’s), conduction aphasia, mixed aphasia, and anomic aphasia. Patients typically exhibit multidimensional impairments in language function, such as non-fluent speech, word-finding difficulties (anomia), simplified grammar, disrupted syntax, impaired auditory comprehension, repetition deficits, alexia, and agraphia, with anomia and impaired repetition being the most commonly observed features[35]. Moreover, individuals with PSA often present with associated cognitive deficits, including impaired executive function, attention, and working memory, which further exacerbate communication difficulties and negatively impact rehabilitation outcomes[42]. Previous studies have demonstrated that early and accurate aphasia subtype classification and functional localization, when combined with individualized speech-language interventions (e.g., constraint-induced therapy, semantic-specific training) and neuromodulation techniques (e.g., transcranial magnetic stimulation, transcranial direct current stimulation), can significantly promote language network reorganization and recovery, improve patients' quality of life, and facilitate social reintegration[12].
Stage-Specific Reorganization of Language Networks
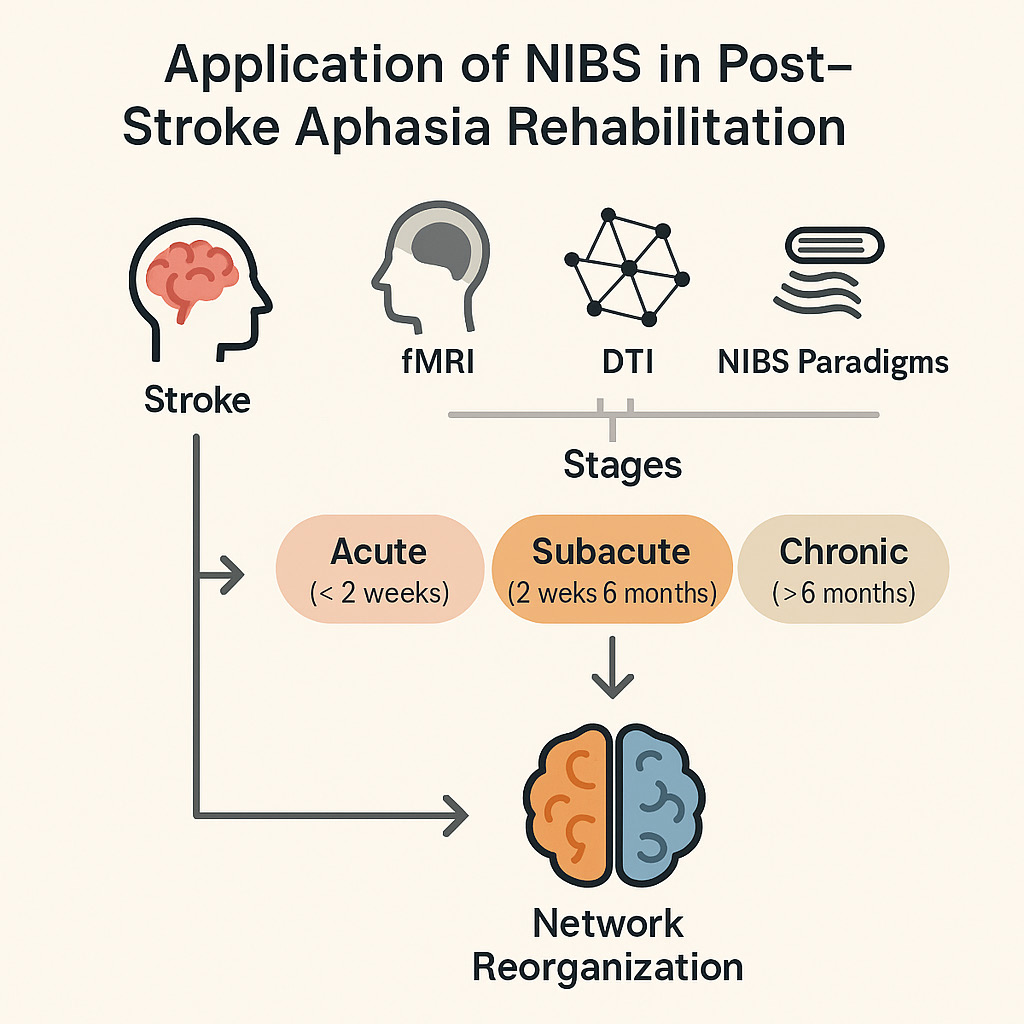
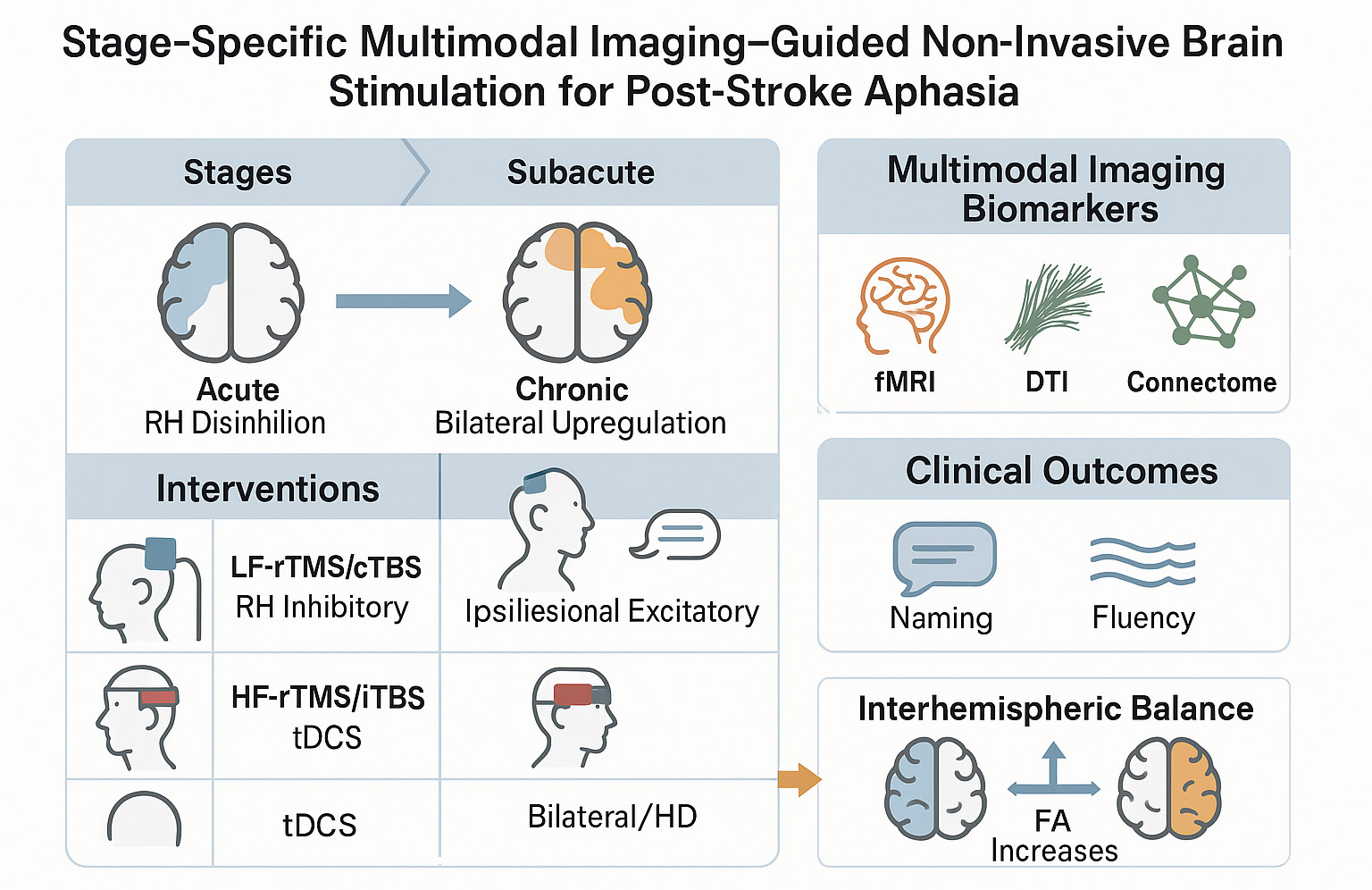
However, the natural recovery of language function in PSA follows a dynamic, three-phase process. Numerous longitudinal functional imaging studies support a triphasic model of language network reorganization encompassing acute, subacute, and chronic stages(Figure 1). During the acute phase (a few days to two weeks post-onset), acute neuronal dysfunction within the lesion site leads to a significant reduction in activation across left-hemispheric language centers—primarily Broca’s area, Wernicke’s area, and the arcuate fasciculus. Simultaneously, interhemispheric inhibition is weakened, resulting in a relative “disinhibition” of contralesional homologous regions in the right hemisphere (RH). However, RH activation during this stage is typically weak and spatially nonspecific. Its role appears preparatory, laying the foundation for subsequent neuroplasticity rather than directly substituting for language functions[19]. In the subacute phase (2 weeks to 6 months post-stroke), partial reperfusion and metabolic recovery within the infarcted area initiate neuroplastic mechanisms such as synaptic remodeling and axonal regeneration. fMRI and positron emission tomography (PET) studies have demonstrated reorganization-related upregulation in both the RH homologous language network (e.g., right Broca–Wernicke circuit) and the residual and perilesional cortex of the left hemisphere. This reorganization is positively associated with early improvements in speech fluency, naming ability, and auditory comprehension and is modifiable through interventions like constraint-induced language therapy (CILT) and neuromodulation[34]. In the chronic phase (>6 months), if the left-hemispheric language network and its subcortical tracts are sufficiently restored, it gradually regains dominance, with activation patterns approaching those of healthy controls. In contrast, persistent RH overactivation, especially in the context of limited left-hemispheric engagement, is associated with poorer long-term outcomes. Predictive models from longitudinal studies suggest that optimal chronic-stage recovery depends more on early preservation of left perilesional cortex and perfusion than on continued RH compensation[19,23,34].
Figure 1. Stage-specific multimodal imaging–guided non-invasive brain stimulation (NIBS) framework for post-stroke aphasia. Multimodal imaging (fMRI, DTI, EEG) delineates dynamic language network reorganization across recovery stages, guiding targeted NIBS strategies. In the acute phase, inhibitory stimulation modulates right-hemisphere hyperactivity; in the subacute phase, bilateral facilitation supports network rebalancing; and in the chronic phase, excitatory stimulation enhances left perilesional plasticity. This framework integrates stage-dependent imaging biomarkers with tailored neuromodulation to optimize individualized language recovery.
Interhemispheric Balance: Facilitation vs. Maladaptation
This triphasic framework highlights the dual role of RH homologous regions: facilitatory disinhibition during early phases, and potentially inefficient compensation during later stages. In acute and subacute phases, RH activation may support early recovery, particularly when the left network is severely impaired. For example, initial gains in language function have been linked to increased activation in the right inferior frontal gyrus and insular cortex[46]. However, in cases where the left hemisphere retains reorganization potential, persistent RH overactivation may disrupt interhemispheric balance and hinder left-sided recovery, negatively affecting long-term prognosis[25,34]. Indeed, sustained RH hyperactivation in the chronic phase has been associated with poorer language performance and increased naming errors[36].
Multiple functional imaging and transcranial stimulation studies have shown that excessive activation in the right hemisphere is often associated with poorer recovery outcomes. Conversely, suppressing such compensatory overactivation—such as through inhibitory transcranial magnetic stimulation (TMS) targeting right-hemispheric homologous regions—may facilitate reorganization of the left-hemispheric language network and improve language performance. This “dual-role” model is commonly conceptualized within the framework of the interhemispheric inhibition model, which posits that early disinhibition of RH circuits may transiently support function, but persistent hyperactivation in the chronic phase may exert maladaptive inhibitory effects on perilesional regions in the left hemisphere. NIBS studies have further validated findings from functional imaging. Evidence indicates that applying inhibitory stimulation to right-hemispheric language areas in patients with chronic PSA can lead to modest improvements in language abilities. While low-frequency repetitive transcranial magnetic stimulation (rTMS) to the RH has demonstrated efficacy in chronic PSA, the optimal time window for intervention is dependent on the patient's recovery phase[20]. Therefore, selecting the ideal intervention window should be guided by multimodal fMRI metrics and standardized language assessment scales.
Aim and Scope of This Structured Narrative Review
In recent years, NIBS—including TMS and tDCS—has emerged as a prominent area of interest in post-stroke aphasia (PSA) rehabilitation due to its favorable safety profile and reproducibility. A growing body of work shows that NIBS can modulate both hemispheric language networks and domain-general control systems, influencing cortical plasticity alongside measurable changes in network function and microstructural architecture. However, the differential efficacy and mechanisms of various stimulation modalities remain incompletely understood. To avoid redundancy, we summarize shared mechanisms once (interhemispheric rebalance; ipsilesional facilitation) and emphasize stage-adapted applications within each modality section below. Multimodal neuroimaging offers a critical window into NIBS-induced functional and structural reorganization, including fMRI, DTI, and high-resolution T1-weighted imaging. Our primary aim is to provide a conceptual, stage-specific synthesis that integrates multimodal imaging with neuromodulation strategies for individualized translation, presenting a structured narrative across fMRI, DTI/structural connectivity, and functional connectivity.
1. Common Non-Invasive Brain Stimulation TechniquesThis section summarizes commonly used NIBS modalities and emphasizes how their mechanisms and optimal applications vary across the acute, subacute, and chronic stages of post-stroke language recovery.
Repetitive Transcranial Magnetic Stimulation: Stage-Adapted OverviewStage-adapted overview. The application and therapeutic efficacy of rTMS in post-stroke aphasia are highly stage-dependent. During the acute phase, low-frequency inhibitory rTMS targeting contralesional homologues may help limit maladaptive hyperexcitability and preserve perilesional function. In the subacute phase, bilateral reorganization predominates; accordingly, either inhibitory stimulation of the right hemisphere or excitatory stimulation of residual left-hemispheric regions can enhance cross-hemispheric balance and promote network reintegration. By the chronic stage, rTMS is primarily used to restore left-dominant activation and reinforce residual perilesional connectivity through excitatory paradigms such as high-frequency rTMS or iTBS. These stage-tailored strategies align with the evolving mechanisms of neural plasticity underlying post-stroke language recovery.
rTMS protocols include conventional stimulation paradigms—such as 1 Hz inhibitory and 10 Hz excitatory protocols—as well as more recent patterned approaches, such as iTBS[7]. For PSA, two primary strategies have been proposed: low-frequency rTMS applied to the right-hemispheric homologous language area to suppress excessive interhemispheric inhibition exerted on the damaged left-hemisphere language network[18,29]; and high-frequency rTMS or iTBS targeting residual language areas in the left hemisphere to directly enhance their functional engagement. Many studies have cited the interhemispheric inhibition hypothesis to explain these effects: following left-hemisphere language network damage, the RH may become hyperactive due to loss of transcallosal inhibition. This hyperactivation may then exert symmetrical inhibition back onto the left hemisphere via the corpus callosum, paradoxically impeding recovery[11,22]. Accordingly, applying low-frequency rTMS to the right Broca’s area homologue can “release the brake” by attenuating right-to-left interhemispheric inhibition, thereby promoting reactivation and reorganization of the left-hemispheric language network[22]. In clinical practice, low-frequency rTMS is typically applied using neuronavigation to localize the right Broca homologue, with a stimulation frequency of 1 Hz, session duration of approximately 20 minutes, and a typical treatment course lasting 1 to 2 weeks. This intervention is often combined with concurrent speech-language therapy and has been shown to significantly improv. For instance, Medina et al. (2012) and Hamilton et al. (2010)[18,29] demonstrated that in patients with, low-frequency rTMS applied to the RH significantly improved discourse productivity and verbal fluency and functional imaging studies suggest that the therapeutic mechanism involves suppression of maladaptive overactivation in the right prefrontal cortex, thereby facilitating re-engagement of left-hemisphere language regions. This neuromodulatory approach remains effective even in the chronic phase of stroke recovery, with evidence supporting sustained clinical benefits for at least six months post-intervention. A study by Harvey et al. (2017)[22] demonstrated that low-frequency rTMS targeting the right Broca homologue can lead to sustained naming improvements in individuals with chronic aphasia. The intervention protocol involved navigated stimulation of the right inferior frontal gyrus (Broca homologue), delivered at 1 Hz for approximately 20 minutes per session over a course of 1–2 weeks. Functional MRI data further revealed that rTMS induced a posterior shift in activation within the right prefrontal cortex—from the anterior part of the Broca homologue (Brodmann area 45) to more motor-related regions (Brodmann areas 6, 44, and 46). Concurrently, there was a significant increase in activation of left-hemispheric regions involved in naming. These findings highlight the potential of rTMS to promote functional reorganization and facilitate long-term language recovery, even in the chronic phase post-stroke, with improvements persisting for at least six months after treatment
High-frequency rTMS or iTBS targeting the left hemisphere is designed to directly strengthen residual language areas and is particularly suited for patients in whom portions of the left-hemispheric language cortex remain functionally intact. Case reports have shown that high-frequency stimulation of the left inferior frontal gyrus or motor-related regions may enhance language output, with neuroimaging evidence indicating improved connectivity within the left-hemispheric language network[49]. However, compared to low-frequency inhibitory stimulation of the right hemisphere, clinical reports on high-frequency rTMS for aphasia are relatively scarce. This is largely due to challenges in precisely targeting intact left-hemispheric regions while avoiding lesioned areas. To address this issue, a personalized targeting approach has recently emerged, integrating functional neuroimaging guidance to identify stimulation sites. Even without navigation equipment, function-specific targets derived from task fMRI can be localized and applied clinically[50]. In a randomized controlled trial, researchers identified language-relevant activation hotspots in the left superior frontal gyrus (SFG) via individual functional imaging and applied rTMS at those targets. Results demonstrated that both excitatory iTBS to the left hemisphere and inhibitory continuous theta-burst stimulation (cTBS) to the right hemisphere, when combined with language therapy, yielded significantly better outcomes than sham stimulation[33]. These findings suggest that non-classical language areas, such as the SFG, may also serve as effective stimulation targets. Notably, high-frequency rTMS, particularly iTBS, offers the advantage of short stimulation durations—approximately 3 minutes per session in the classical iTBS protocol—thus imposing minimal burden on patients. However, to consolidate treatment effects, extended stimulation protocols or increased session counts may be required.
Moreover, large-sample studies and systematic reviews have provided higher levels of evidence supporting the use of rTMS in the treatment of aphasia. A recent systematic review and meta-analysis included 47 randomized controlled trials (RCTs) involving 2,190 patients with non-fluent aphasia, and demonstrated that rTMS significantly improves post-stroke language function, including abilities in repetition, naming, and spontaneous speech. Severity scores for aphasia were significantly reduced, and some studies also reported increased serum brain-derived neurotrophic factor (BDNF) levels and reduced depression incidence in the rTMS groups[7]. Another double-blind RCT targeting chronic non-fluent aphasia applied 1 Hz low-frequency rTMS to the right inferior frontal gyrus (triangular part), combined with multimodal aphasia therapy (M-MAT). Compared to the sham stimulation + training group, the real rTMS + training group showed an additional improvement of approximately 4.6 points in the WAB Aphasia Quotient at 15-week follow-up. Patients who received rTMS exhibited fewer word-finding difficulties and produced longer, more complete sentences. The study was graded as Class III evidence by Neurology, suggesting that rTMS may provide additional therapeutic benefit when used as an adjunct to conventional speech-language training[27]. Taken together, the overall efficacy of rTMS for aphasia has been supported by multiple randomized controlled trials.
Nevertheless, significant variability exists across rTMS protocols, and some findings are even contradictory. For example, low-frequency inhibitory stimulation of the right hemisphere may have limited efficacy in certain patients—such as those with severe global aphasia—in whom right-hemispheric compensation may still be contributing to residual language function; in such cases, excessive suppression of the RH may be counterproductive. Conversely, high-frequency stimulation of the left hemisphere requires the presence of sufficient residual functional cortex, which may be lacking in patients with extensive left-hemispheric lesions, limiting its utility[11]. In addition, there is considerable inter-individual variability in brain network reorganization patterns following stroke, making it a current challenge—and research focus—to personalize rTMS parameters and stimulation targets based on lesion location and recovery stage.
Theta Burst Stimulation: intermittent TBS and continuous TBSThe rationale for using TBS in post-stroke aphasia also follows a stage-specific pattern. In the early acute stage, cTBS may suppress maladaptive contralesional overactivation and prevent inhibitory dominance from the right hemisphere. During the subacute period, excitatory iTBS[24] over perilesional or residual left-hemispheric areas can amplify ongoing neuroplastic changes and facilitate bilateral reorganization. In the chronic stage, TBS protocols are increasingly employed to strengthen stable left-hemispheric circuits and consolidate language network re-engagement, often in combination with behavioral language training. iTBS [24] is a rapid pattern of rTMS that delivers short bursts of high-frequency pulses at a theta rhythm (~5 Hz). Each burst consists of three 50 Hz pulses, repeated every 200 milliseconds (i.e., at 5 Hz). A standard iTBS protocol includes 2 seconds of stimulation followed by 8 seconds of rest, repeated in cycles for a total of approximately 190 seconds, delivering 600 pulses in total. Stimulation intensity is typically set at 80% of the active motor threshold (AMT). This rhythmic alternation is believed to induce theta-frequency brain oscillations, which may simulate endogenous cortical rhythms and regulate activity within neural networks[39]. iTBS exerts excitatory effects on the cortex and is commonly used to enhance excitability in the lesioned language areas of patients with aphasia. The target region is usually the posterior inferior frontal gyrus (Broca’s area) in the left (dominant) hemisphere, aiming to enhance both local and network-level activation. A randomized controlled trial by Bai et al. (2025) confirmed that iTBS combined with language training significantly improves language production functions in patients with post-stroke aphasia, including spontaneous speech, naming, and repetition, as well as increasing the Aphasia Quotient (AQ)[2]. The study revealed that, compared to baseline, patients in the iTBS group showed significant improvements in all aforementioned language domains, with gains in naming, repetition, and AQ significantly greater than in the sham-stimulation group. Further fMRI analyses suggested a potential mechanism: resting-state fMRI comparisons before and after treatment revealed significant increases in fractional amplitude of low-frequency fluctuations (fALFF)[44] and degree centrality in several language-related areas of the left frontal and temporal lobes. These findings indicate that iTBS may strengthen the activation and network centrality of left-hemisphere language circuits, thereby enhancing functional connectivity efficiency and supporting language recovery. Consequently, promoting neuroplasticity within the lesioned (left) hemisphere is regarded as a key mechanism by which iTBS facilitates language rehabilitation. Through rhythmic stimulation, iTBS induces localized neuronal excitation and network reorganization, thereby reinforcing residual left-hemispheric language activity and facilitating functional restoration. Moreover, some studies have observed that iTBS can entrain theta-frequency neural oscillations that persist for several hundred milliseconds after stimulation, suggesting that iTBS may “imprint” frequency-specific rhythms into brain networks[39]. These oscillations may facilitate the modulation of speech-related cognitive processes, offering an additional explanatory pathway for the therapeutic benefits of iTBS in aphasia.
cTBS shares the same fundamental stimulation unit as iTBS—namely, bursts of three 50 Hz pulses—but is delivered continuously without interruption. A typical cTBS protocol administers 600 pulses over approximately 40 seconds (i.e., 200 bursts delivered consecutively without intervals), with stimulation intensity set at 80% of the active motor threshold (AMT). In contrast to iTBS, cTBS produces an inhibitory aftereffect on cortical excitability: a single session of cTBS can result in reduced excitability of the target cortex lasting up to 60 minutes[3]. Clinically, cTBS is commonly employed to suppress hyperactivity in the contralesional (right) hemisphere, particularly in language-homologous regions, to rebalance interhemispheric inhibition. For instance, cTBS may be targeted to the right posterior superior temporal gyrus (pSTG)—the homolog of Wernicke’s area—or to the right pars triangularis—the counterpart of Broca’s area—to reduce compensatory overactivation in these areas and release inhibitory pressure on the left-hemispheric language network. This approach is grounded in the interhemispheric imbalance model of post-stroke recovery, which posits that damage to the left-hemispheric language areas often leads to compensatory overactivation in the right hemisphere. This right-sided hyperexcitability, in turn, exerts excessive transcallosal inhibition on the left hemisphere, thereby impairing recovery of language functions[5,24]. By suppressing the overactive right hemisphere with cTBS, a more favorable environment is created for functional reorganization in the left hemisphere. Empirical evidence supports this mechanism. In a randomized controlled trial, Zheng et al.[48] applied cTBS to the right pSTG (homologous to Wernicke’s area) in patients with post-stroke aphasia and found significant improvements in auditory comprehension and repetition. Functional imaging revealed a notable reduction in overactivation of the right pars triangularis, along with increased spontaneous neural activity in the left frontal lobe. These findings suggest that suppressing hyperactivity in right-hemispheric language regions reduces their interference with left-hemispheric language circuits, thereby enhancing cortical activation in the lesioned hemisphere and facilitating functional recovery. Further support comes from a study by Harvey et al.[21], who applied cTBS to the right pars triangularis in patients with chronic aphasia. The intervention led to notable improvements in object naming, primarily by reducing errors related to phonological access deficits. The authors proposed that right-sided cTBS facilitated the phonological encoding stage, thereby enhancing the retrieval of word forms in these patients. These findings highlight the potential of cTBS to modulate maladaptive neural activity in the right hemisphere and support targeted interventions based on the specific nature of language impairments, such as phonological deficits in naming.
Notably, the short-term effects of cTBS are not limited to local changes in cortical excitability but also extend to the modulation of network connectivity. Yoo et al. conducted a study using combined transcranial magnetic stimulation and electroencephalography (TMS-EEG) to examine network-level effects of cTBS in healthy participants[43]. Neuronavigated cTBS was delivered to the left pars opercularis—a subregion of Broca’s area—and the researchers observed a significant enhancement of phase synchrony between bilateral Broca areas in the gamma frequency band (250–350 ms time window). In addition, increased intrahemispheric synchrony was detected between the left pars opercularis and other left-hemisphere language-related regions (e.g., left supramarginal gyrus, left superior temporal gyrus) in both the gamma and theta/delta bands across various time windows. In contrast, the sham stimulation group exhibited no such increases in synchrony; in some cases, synchrony even decreased in specific frequency bands. These findings suggest that cTBS can modulate both inter- and intrahemispheric connectivity within the language network, facilitating coordinated activity between bilateral language areas as well as enhancing intra-network synchrony within the left hemisphere. This modulation of network dynamics indicates that cTBS may promote language recovery by reorganizing the temporal and spatial architecture of the language system. In addition, a recent systematic review summarized all available RCTs investigating TBS for post-stroke functional deficits[24]. The review concluded that TBS exhibits a favorable trend toward superior rehabilitation outcomes compared to conventional rTMS, across multiple domains including motor recovery, aphasia, and spatial neglect. Specifically, iTBS enhances cortical excitability in the lesioned hemisphere to promote functional restoration, while cTBS suppresses excessive contralesional activity to restore network balance.
In summary, TBS represents a powerful neuromodulatory tool for language network reorganization in post-stroke aphasia. Compared to conventional rTMS, TBS offers advantages such as lower stimulation intensity, shorter administration time, and longer-lasting aftereffects[24]. However, due to the limited number and heterogeneity of existing studies, there is currently insufficient evidence to recommend a single optimal TBS protocol. Variability in stimulation targets, dosages, and timing across studies has led to inconsistent efficacy outcomes. Therefore, future research should focus on large-scale, high-quality multicenter RCTs, combined with multimodal neuroimaging assessments, to determine the most effective stimulation parameters and optimal intervention windows for TBS in aphasia rehabilitation.
Transcranial Direct Current StimulationtDCS is a non-invasive brain stimulation technique that modulates cortical excitability through the application of low-intensity direct current. Compared with TMS, tDCS devices are more compact and portable, and the stimulation procedure is simpler, making tDCS a widely used intervention in aphasia rehabilitation. The method involves placing a pair of electrodes (anode and cathode) on the scalp to deliver a constant low current that subtly alters neuronal membrane potentials. Cathodal stimulation typically leads to membrane hyperpolarization and decreased excitability, while anodal stimulation induces depolarization and increased excitability of the underlying cortex[4,17,37]. In the treatment of post-stroke aphasia, the most common electrode configuration is bilateral tDCS, which aims to restore interhemispheric balance. Typically, the anode is positioned over the left inferior frontal gyrus (Broca’s area) or the left primary motor cortex (M1) to enhance excitability of the lesioned hemisphere, while the cathode is placed over the homologous region on the right hemisphere (e.g., right Broca’s area or right M1) to suppress contralesional overactivity[37]. This approach mirrors the interhemispheric modulation model employed in rTMS, combining excitation of the lesioned side with inhibition of the intact side. In post-stroke aphasia interventions, a commonly employed electrode montage for tDCS is the "bilateral-balanced" configuration, in which the anode is placed over the left inferior frontal gyrus (Broca’s area) or the left primary motor cortex (M1) to enhance excitability of the lesioned hemisphere’s language center, while the cathode is positioned over the corresponding area in the contralateral hemisphere (right Broca’s homolog or right M1) to suppress excitability in the intact hemisphere. This approach aims to achieve a balanced modulation of hemispheric excitability, mirroring the strategy of "inhibiting the contralesional side and exciting the ipsilesional side" commonly used in rTMS protocols[15,16,32]. For instance, Soliman et al. applied anodal stimulation over the left Broca’s area and cathodal stimulation over the right Broca’s homolog, and demonstrated that this bilateral tDCS montage could promote language recovery in patients with aphasia[37]. tDCS is commonly administered in conjunction with language training, typically for 20 minutes per session, once daily for 1–2 weeks (approximately 10 sessions). During stimulation, patients perform naming, repetition, or other language-related tasks. This simultaneous training leverages the neuroplastic “window of opportunity” induced by tDCS, allowing the therapeutic effects of training to be more effectively integrated into functional brain networks. Multiple studies, including randomized controlled trials, have shown that tDCS combined with behavioral training yields more significant and lasting improvements in language function than behavioral training alone. For example, Meinzer et al. conducted a double-blind RCT involving patients with chronic aphasia and found that applying anodal tDCS over the left M1 (twice daily, 20 minutes each session) at the start of each intensive naming session over a two-week period significantly enhanced naming performance for trained words. Moreover, the improvement generalized to untrained vocabulary, and performance remained stable at 6-month follow-up in the tDCS group, whereas the sham group exhibited partial decline. Naming accuracy for untrained words also improved significantly only in the tDCS group, with no change in the control group. Functional communication skills, such as conversational ability, were likewise significantly better in the tDCS group[30]. This study provided the first RCT evidence demonstrating that tDCS not only improves core language functions (e.g., naming accuracy) but also facilitates long-term retention and generalization of therapy outcomes. In other words, tDCS accelerates immediate language recovery while promoting broader network plasticity that supports sustained and generalized language improvement following the end of training.
From a neuroimaging perspective, the effects of tDCS on the brain of patients with aphasia can be described as “broad yet subtle” modulation. On one hand, tDCS reduces unnecessary overactivation in non-language regions; on the other hand, it enhances the coordinated activity within language-related networks. Darkow et al[10]. investigated the immediate effects of tDCS on brain activity in aphasic patients using concurrent fMRI. Compared to sham stimulation, anodal tDCS over the left hemisphere significantly reduced task-related overactivation in higher-order cognitive control areas unrelated to naming (suggesting suppression of these “interfering” regions), while activation within the core language network—primarily the left frontal, temporal, and parietal areas—increased. Functional connectivity analyses further revealed increased low-frequency synchronization within the language network, indicating more efficient communication among its constituent nodes. In a 6-week extended intervention, Cherney et al. (2021) demonstrated that both anodal and cathodal fMRI-guided tDCS combined with language therapy led to greater improvements in functional language and clinical ratings compared to therapy alone. Notably, cathodal stimulation was associated with increased perilesional cortical activation[8]. Taken together, these findings suggest that tDCS may function by “reducing noise and amplifying signal”—that is, by suppressing extraneous brain activity unrelated to language processing while simultaneously enhancing the functional coupling within language-relevant areas, thereby creating a more optimized neural environment for language processing. Beyond changes in functional activity, structural plasticity induced by tDCS has also been reported. In a DTI study, Soliman et al.[37] found that short-term repeated tDCS led to observable plastic changes in white matter tracts involved in language. Specifically, they reported a significant post-treatment increase in the fractional anisotropy (FA) of the right uncinate fasciculus (UNC)—a major white matter tract connecting the temporal and frontal lobes, including key language regions. This suggests that tDCS may promote remodeling of white matter and myelin integrity, thereby enhancing structural connectivity within and between hemispheric language areas. Interestingly, in that study, although the electrode was placed over the left hemisphere, the observed white matter changes were predominantly in the right hemisphere. The authors hypothesized that left-hemisphere stimulation may have modulated contralateral regions via interhemispheric networks—indicating that tDCS can promote bilateral cooperative plasticity. Unlike TMS, which directly induces excitatory neural firing, tDCS exerts a gentler influence. It operates with low current intensity and broad diffusion, without immediately triggering neuronal discharges. However, it is precisely this low-intensity, sustained modulation—especially when paired with behavioral training—that enhances the plastic potential of neural circuits. This enables the brain to reorganize its networks in a “quietly guided” manner. Rather than directly replacing impaired language functions, tDCS elevates the brain’s baseline capacity for executing language tasks. It thereby increases the efficiency of language processing and allows patients to derive greater and more enduring benefits from subsequent language therapy.
In recent years, several modified transcranial electrical stimulation techniques—such as high-definition transcranial direct current stimulation (HD-tDCS) and transcranial alternating current stimulation (tACS)—have been introduced into the field of aphasia rehabilitation. These methods aim to achieve more precise or deeper neuromodulation by altering electrode configurations or current waveforms. However, current evidence regarding their use in aphasia remains limited, and their clinical efficacy requires further validation. Notably, while traditional approaches emphasize suppression of the right hemisphere to relieve its inhibitory effect on the lesioned left hemisphere, some studies have proposed alternative strategies. For patients with extensive left-hemispheric lesions and minimal residual language network capacity, enhancing right hemisphere activity may serve as a compensatory approach. A recent meta-analysis[51] evaluated the effect of anodal tDCS applied to the right hemisphere on naming performance in individuals with post-stroke aphasia. The results indicated that patients receiving right-anodal tDCS demonstrated a greater trend toward improvement in naming accuracy compared to those receiving sham stimulation or conventional therapy. Based on these findings, the authors suggested that anodal stimulation over the right hemisphere could be a promising intervention, particularly in cases where the left-hemispheric language areas are severely damaged. This view diverges somewhat from the classic "right-suppression" model. The study proposed that right-hemisphere anodal tDCS may serve as a compensatory adjunct for patients with large left-sided lesions and limited residual plasticity. However, for patients with a partially preserved left-hemispheric language network, left-sided stimulation should remain the priority, while prolonged right-hemisphere overactivation should be avoided. In addition, several studies have focused on bihemispheric tDCS protocols, which combine anodal stimulation to the left hemisphere with cathodal stimulation to the right, aiming to concurrently increase left-hemispheric excitability while suppressing right-sided overactivation[13]. More recently, a novel tDCS approach has targeted the right cerebellum for aphasia treatment[28]. Meta-analytic evidence shows that cerebellar TMS improves balance and limb motor outcomes and modulates motor-related rs-fMRI networks, indicating that cerebello-cortical circuits are plastic and may serve as analogues for cross-network interventions in language recovery[45]. This region has both structural and functional connections with the left-hemispheric language areas, which is particularly important in patients with large left-hemisphere lesions where it may be difficult to identify viable perilesional cortex for direct stimulation.
tDCS: Stage-Specific Considerations and Take-Home MessageIn summary, tDCS offers a safe and feasible “foundational modulation” strategy for post-stroke aphasia. By balancing cortical excitation and inhibition and promoting neural network reorganization, tDCS exerts a mild yet profound influence on the remodeling of the language network, thereby creating a more favorable neural environment for language rehabilitation. Looking ahead, as stimulation parameters are further optimized and integrated with neuroimaging and physiological markers, it may become possible to more precisely identify suitable candidates for tDCS and develop personalized stimulation protocols. Such advances are expected to enhance the efficacy of tDCS and broaden its application in aphasia rehabilitation. The therapeutic role of tDCS also evolves across recovery stages. In the acute phase, early bilateral or contralesional-anodal montages may facilitate global excitability and prevent network diaschisis. The subacute phase benefits most from bihemispheric configurations that balance interhemispheric inhibition and enhance task-specific learning when paired with speech therapy. In the chronic phase, left-anodal or bilateral tDCS targeting residual cortical regions promotes long-term restoration of left-dominant network integrity. These temporal shifts underscore the importance of stage-adapted stimulation paradigms within a precision neuromodulation framework.
Functional MRI Evidence of NIBS-Induced Reorganization
fMRI has been widely used to measure changes in brain activation and network connectivity before and after NIBS. Multiple small-sample studies have demonstrated that interventions using TMS or tDCS can induce plastic reorganization of functional activation patterns in the brain.
Immediate and Short-Term Effects: iTBS, a highly efficient TMS protocol, can induce immediate changes in brain function after a single session of intervention[38]. Xu et al. (2021) [41]applied a single session of iTBS over the left primary motor cortex (M1) in 16 patients with post-stroke aphasia, followed by resting-state fMRI immediately before and after stimulation. The results showed significant changes in local neural activity and functional connectivity after a single session of iTBS: degree centrality increased in the right middle frontal gyrus and left parietal lobe, while fractional amplitude of low-frequency fluctuations decreased in parts of the frontal and occipital lobes, and functional connectivity between the left M1 and the left superior frontal gyrus weakened. These findings suggest that even a single session of TMS can modulate brain network activity acutely, providing insights into how to facilitate language network plasticity and laying a neurophysiological foundation for subsequent language rehabilitation training.
Concurrent Stimulation-Imaging Studies: Darkow et al. (2017) conducted a simultaneous tDCS-fMRI study using a double-blind crossover design, in which patients with chronic aphasia received either real or sham tDCS during a naming task inside the MRI scanner. Results showed that anodal stimulation reduced over-reliance on higher-order cognitive control regions during naming, enhanced activation within the core language network, and promoted low-frequency oscillations. Furthermore, the functional activation patterns of patients receiving real stimulation became more similar to those of healthy controls[10].
These results indicate that a single session of tDCS can modulate residual language networks in aphasia, reduce unnecessary cognitive control, and enhance intra-network coordination—providing a potential mechanism for subsequent individualized behavioral interventions.
Long-Term Reorganization Effects: fMRI has also been employed to investigate lasting functional reorganization following repeated NIBS interventions. For example, a protocol using low-frequency rTMS to inhibit the right inferior frontal gyrus (IFG) has been applied to reduce maladaptive right-hemisphere compensation, aiming to release suppressed functions of the left-hemisphere language areas. Harvey et al. (2017)[22] applied 1 Hz rTMS to the right IFG pars triangularis (homologous to Broca's area) in 9 patients with chronic aphasia for 10 consecutive days. Naming performance improved significantly, peaking at 6-month follow-up. Corresponding fMRI revealed a posterior shift in activation within the right IFG: whereas naming-related activation was localized to BA45 (pars triangularis) before intervention, this region was no longer active after 6 months. Instead, activation appeared in more posterior right IFG subregions, such as the pars opercularis (BA6/44/46). Furthermore, activation patterns shifted from right-hemisphere dominance to increased involvement of left-hemisphere regions, including the supplementary motor area, medial frontal cortex, and cingulate gyrus. In other words, rTMS promoted a shift in compensatory activation within the right frontal cortex from anterior (BA45) to posterior areas (BA6/44/46), along with increased recruitment of the left hemisphere—reflecting a dynamic reorganization of the bilateral language network. These changes coincided with sustained language improvement, supporting the therapeutic strategy of reducing excessive right frontal compensation while enhancing left-hemisphere engagement. Similarly, in a study by Chang et al. (2022)[6], high-frequency rTMS was delivered to the most active residual left-hemisphere language region identified by functional near-infrared spectroscopy (fNIRS), combined with 10 days of speech therapy in 5 patients with chronic non-fluent aphasia. Significant improvement in the Aphasia Quotient (WAB) was observed within one month. Network analysis using fNIRS showed enhanced functional connectivity among left-hemisphere speech production and processing areas, with significantly increased local clustering coefficients. In contrast, the clustering coefficient in the right hemisphere decreased, slightly reducing global network efficiency. This suggests that enhancing left-hemisphere integration while reducing maladaptive right-hemisphere compensation may be a mechanism for language recovery.
Numerous neuroimaging studies have demonstrated that the mechanisms underlying language recovery align with existing theories of neural plasticity. Patients with better outcomes often exhibit reestablishment of left-hemisphere language network dominance, while right-hemisphere compensation is either suppressed (e.g., via low-frequency rTMS to reduce interhemispheric inhibition) or reorganized into a more supportive role (e.g., posterior shift of compensatory activation to more efficient regions)[19,22]. These neuroplastic changes are often observed concurrently with improvements in language performance, suggesting that the restoration of function is indeed grounded in reorganization of the brain’s language network. Conversely, patients who fail to exhibit such neuroimaging-based markers of plasticity often show limited language improvement. When clinical gains are not paralleled by expected imaging changes, this may indicate the need for adjusting stimulation strategies to optimize treatment efficacy.
Most of the aforementioned fMRI studies are small-scale pre-post comparisons or preliminary RCTs, with sample sizes ranging from fewer than 10 to approximately 20 participants, and some incorporating sham stimulation as controls[37]. Despite these limitations, the findings consistently demonstrate that NIBS can induce favorable functional reorganization of the brain—characterized by increased activation and connectivity in left-hemisphere (ipsilesional) language regions and reduced maladaptive overactivation in the right hemisphere (contralesional), thereby aligning brain activity patterns more closely with those seen in healthy language networks. Such functional neuroimaging evidence provides a mechanistic foundation supporting the use of NIBS to facilitate aphasia recovery. Nonetheless, given the heterogeneity of participants and methodological constraints, these conclusions require further validation in large-scale, rigorously designed clinical trials.
Structural Imaging Studies: White Matter and Gray Matter Plasticity
White Matter PlasticityDTI has been primarily used to assess the structural integrity and connectivity of white matter (WM) fiber tracts, offering a unique perspective on plasticity induced by brain stimulation. Compared with fMRI, which reflects functional changes, DTI reveals remodeling of the underlying anatomical connections within the neural network. Soliman et al. (2021)[37] conducted a randomized trial in 21 subacute post-stroke aphasia patients, comparing a real tDCS group (anodal over the left inferior frontal gyrus [IFG], cathodal over the right IFG) and a sham group, both receiving 10 sessions of stimulation. While the sham group showed no significant language changes, the real tDCS group demonstrated marked improvement in HSS aphasia scores. Seven patients in the real tDCS group underwent pre- and post-intervention DTI scans. Tractography of language-related white matter bundles revealed that, compared with sham stimulation, real tDCS significantly increased FA in the right uncinate fasciculus and decreased mean diffusivity (MD) in the right fronto-insular tract—suggesting enhanced fiber integrity and reduced extracellular diffusivity. Notably, the increase in FA of the right uncinate fasciculus positively correlated with gains in speech fluency, supporting the idea that greater structural remodeling parallels greater functional recovery. Zhao et al. (2021)[47] examined 39 patients with primary progressive aphasia (PPA) who received 15 sessions of naming therapy combined with left IFG tDCS, and analyzed DTI metrics of ventral (uncinate/inferior longitudinal fasciculi) and dorsal (arcuate fasciculus) pathways prior to intervention. Their results showed that the tDCS group outperformed the sham group in naming accuracy for both trained and untrained words. Higher FA in ventral pathways predicted greater gains in trained items, while higher FA in dorsal pathways predicted better generalization to untrained words. This suggests that the structural integrity of language-related WM tracts may serve as a predictive biomarker of therapeutic responsiveness to tDCS in PPA patients—those with more preserved WM structures tended to benefit more from stimulation. Allendorfer et al. (2012)[1] reported that following 10 days of excitatory iTBS over the left hemisphere in chronic aphasia patients, FA significantly increased in several left-hemispheric regions, including the inferior and superior frontal gyri and the anterior corpus callosum. Additional FA increases were observed in the right midbrain, bilateral temporoparietal cortex, and posterior cingulate gyrus, whereas decreases appeared in the bilateral fusiform gyri and left cerebellum. These changes overlapped with activation regions identified in previous fMRI studies of iTBS-induced language facilitation, suggesting that excitatory rTMS may enhance synaptic connectivity via mechanisms such as long-term potentiation (LTP), which is reflected structurally as improved WM integrity. Recent studies combining NIBS and language therapy have also reported microstructural WM plasticity in perilesional or contralesional tracts, such as increased FA or decreased MD in the right uncinate and fronto-insular fasciculi following bilateral tDCS[37]. These structural changes have been closely linked to improvements in speech fluency. Collectively, these findings highlight the parallel nature of structural and functional plasticity, supporting the concept that NIBS facilitates coordinated reorganization at both anatomical and functional levels of the language network.
Gray Matter PlasticityAlthough relatively fewer studies have focused on gray matter (GM) volume changes, emerging evidence suggests a link between GM remodeling and functional language recovery. Some studies have reported that increased GM volume in the right temporoparietal junction is significantly associated with improved language outcomes in post-stroke aphasia patients—even though this region lies in the contralesional hemisphere and is not homologous to the lesioned left-hemispheric language areas[40]. This finding implies that cortical GM remodeling—such as hypertrophy in language-related regions of the intact hemisphere—may also represent a form of neuroplasticity that contributes to compensatory mechanisms supporting language recovery.
Integrated Multimodal Imaging Framework for Stage-Specific Neuromodulation
Based on the synthesis of multimodal neuroimaging findings, Han et al. (2024)[19] proposed a plasticity framework of the post-stroke language network grounded in the dual-stream model, providing a systematic summary of recovery mechanisms across different stages. They mapped specific white matter pathways—such as those related to fluency, repetition, comprehension, naming, and reading—to corresponding subcomponents of language, highlighting the plasticity characteristics of these tracts during recovery. The model emphasizes that in the acute stage, due to severe functional disruption in the lesioned left hemisphere and limited capacity for white matter reconstruction, language recovery relies predominantly on functional reorganization within residual cortical areas and perilesional zones. In the subacute phase, with the initiation of neuroplastic and metabolic processes, compensatory remodeling can be observed in both the right-hemispheric homologous pathways and left perilesional networks, supporting intermediate-term functional gains. In the chronic phase, if the left hemisphere gradually regains its dominance in the language network, the global activation pattern tends to normalize and resemble that of healthy individuals. Conversely, persistent over-reliance on right-hemispheric pathways—although offering temporary compensation—may suppress more efficient reorganization in the left hemisphere, leading to suboptimal outcomes. The framework also advocates for dynamic monitoring using multimodal imaging at different recovery stages, and stresses the importance of tailoring the timing and targets of intervention. For instance, the authors identified regions such as the medial superior frontal gyrus and dorsal anterior cingulate cortex as promising neuromodulatory targets due to their involvement in higher-order cognitive control networks. However, multi-target stimulation did not outperform optimized single-target stimulation; notably, rMFG targeting effectively downregulated dACC activity[14]. This conceptual model provides a structured guideline for future clinical decision-making and study design; however, its assumptions warrant further validation through longitudinal and multimodal interventional research. Collectively, these multimodal imaging findings not only delineate the dynamic reorganization of post-stroke language networks but also provide a practical rationale for tailoring NIBS interventions. Functional hypoactivation and interhemispheric imbalance identified through fMRI, together with DTI-derived measures of tract integrity, can inform the selection of stimulation targets, polarity, and timing across different recovery stages, thereby establishing a clinically meaningful imaging-guided neuromodulation framework.
Future Directions and Perspectives
Future research on NIBS for aphasia should focus on several key directions to further enhance its therapeutic efficacy and translational relevance. Despite encouraging progress, significant challenges remain, including the lack of standardized imaging biomarkers, small sample sizes, heterogeneous stimulation timing and parameters, and limited reproducibility across studies. Addressing these limitations will be essential for achieving methodological consistency and clinical generalizability.
First, integrating multiple neuroimaging modalities—such as fMRI, DTI, and electroencephalography (EEG)—is essential for dynamically monitoring the remodeling of language networks and capturing both functional and structural changes during recovery. EEG, with its high temporal resolution, can complement MRI-based approaches by revealing real-time oscillatory and network-level changes induced by stimulation, thereby improving the temporal precision of multimodal imaging frameworks. Such multimodal fusion will enable real-time assessment of neuroplasticity induced by NIBS and facilitate a deeper understanding of the neural signatures associated with each recovery stage.
Second, the application of machine learning and artificial intelligence techniques should be expanded to comprehensively analyze patients’ baseline neuroimaging and clinical data. This approach allows for predictive modeling of language recovery trajectories and supports the optimization of individualized intervention strategies. Data-driven models that incorporate structural and functional MRI, as well as DTI parameters, can estimate patient-specific responsiveness to different stimulation paradigms and assist in evidence-based decision-making[9].
Third, the development of personalized NIBS protocols that adapt to each patient’s stage of recovery—guided by predictive models and imaging biomarkers—could align stimulation intensity and pattern with the evolving neuroplastic potential of the brain. A phase-specific, progressive stimulation strategy may maximize functional gains and improve the long-term stability of outcomes.
In addition to the well-established TMS and tDCS paradigms, several emerging neuromodulation techniques—including transcranial alternating current stimulation, transcranial random noise stimulation, and focused ultrasound neuromodulation—are gaining increasing attention for their potential to deliver more frequency-specific, spatially precise, and depth-selective modulation of neural activity. Although empirical evidence in post-stroke aphasia remains limited, incorporating these novel modalities into multimodal imaging–guided frameworks represents a promising frontier for advancing precision neuromodulation. Future research should explore how these innovative stimulation techniques can be integrated with neuroimaging and computational modeling to improve personalization and reproducibility in language rehabilitation.
Finally, translating neuroimaging-based mechanistic insights into standardized clinical protocols remains a critical challenge. Large-scale, multicenter trials are needed to establish consensus on stimulation parameters, timing, and intervention paradigms, thereby facilitating integration into routine clinical practice. Developing standardized imaging biomarkers and reproducible stimulation frameworks will be crucial for bridging the gap between mechanistic studies and clinical application. Bridging the gap between experimental and clinical implementation will depend on the development of replicable, guideline-based NIBS frameworks that ensure accessibility, consistency, and clinical benefit across diverse patient populations[9]. Future studies should also integrate molecular biomarkers such as BDNF and synaptic plasticity indices with multimodal imaging metrics to better elucidate how cellular mechanisms translate into macroscopic network reorganization and clinical improvement.
Evidence Synthesis and Consistency Across Studies
Although considerable heterogeneity exists among study designs, stimulation parameters, and imaging methods, several consistent patterns have emerged. Across multiple pilot and randomized controlled trials, inhibitory NIBS applied to right-hemispheric homologues and excitatory stimulation targeting left perilesional or residual language areas have repeatedly demonstrated beneficial effects) on naming, fluency, and comprehension[7,33]. Meta-analyses[7] further support the superiority of bihemispheric or imaging-guided protocols compared to conventional approaches. However, controversies remain regarding the optimal timing of stimulation, the durability of long-term effects, and inter-individual variability in response patterns[19]. Overall, the level of evidence has progressed from small-scale exploratory studies to a growing number of well-controlled clinical trials, reflecting an encouraging trend toward standardization and higher methodological rigor.
Conclusion
In summary, non-invasive brain stimulation offers renewed hope for post-stroke aphasia rehabilitation, while multimodal neuroimaging provides a powerful means to elucidate its mechanisms and therapeutic effects. Recent evidence shows that NIBS can promote neuroplastic changes at multiple levels—from the reorganization of functional networks to potential strengthening of structural pathways. Nonetheless, it is increasingly evident that each patient’s path to recovery is unique, requiring more precise and individualized intervention strategies. Future advances in neuroimaging and data analytics are expected to further refine our understanding of language network remodeling, enabling clinicians to design more targeted, stage-specific treatment plans. With continued scientific exploration, the field is moving toward a more complete blueprint of language recovery, offering tangible improvements in communication ability and quality of life for patients with aphasia.
Abbreviations
NIBS=Non-invasive brain stimulation; TMS=Transcranial magnetic stimulation; rTMS=Repetitive transcranial magnetic stimulation; TBS=Theta burst stimulation; iTBS=Intermit-tent theta burst stimulation; cTBS=Continuous theta burst stimulation; tDCS=Transcranial direct current stimulation; HD-tDCS=High-definition transcranial direct current stimu-lation; tACS=Transcranial alternating current stimulation; PSA=Post-stroke aphasia; RH=Right hemisphere; fMRI=Func-tional magnetic resonance imaging; DTI=Diffusion tensor im-aging; PET=Positron emission tomography; fNIRS=Functional near-infrared spectroscopy; EEG=Electroencephalography; IFG=Inferior frontal gyrus; SFG=Superior frontal gyrus; pST-G=Posterior superior temporal gyrus; BA=Brodmann area; M1=Primary motor cortex; AQ=Aphasia Quotient; WAB=West-ern Aphasia Battery; CILT=Constraint-induced language thera-py; M-MAT=Multimodal aphasia therapy; BDNF=Brain-derived neurotrophic factor; PPA=Primary progressive aphasia; FA=-Fractional anisotropy; MD=Mean diffusivity; UNC=Uncinate fasciculus; CC=Corpus callosum; WM=White matter; GM=Gray matter; AI=Artificial intelligence; RCT=Randomized controlled trial.
Declarations
Author Contributions
Liting Chen: Conceptualization, literature search, data compila-tion, manuscript drafting. Zhenye Luo: Literature search, data analysis, manuscript drafting. Xiaoling Wu: Literature search support, figure/table preparation. WenYing Chen: manuscript revision. Xiaole Fan: Project supervision, study design, final manuscript approval.
Acknowledgment
We acknowledge the participants of our study for their contri-bution and our team members for their support.
Funding Information
We acknowledge financial support from the Medical Science and Technology Research Fund of Guangdong Province, China (No. A2023144) and Guangdong Provincial Young Innovative Talents Project (Grant No. 2025KQNCX005).
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Jinan University (Approval No. KY-2024-096).
Competing Interests
Competing financial interests: The authors declare no compet-ing financial interests.
Data Availability
No new datasets were generated or analyzed in this review article. All data cited in this manuscript are from previously published studies, which are properly referenced in the text.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Stage-specific multimodal imaging–guided non-invasive brain stimulation (NIBS) framework for post-stroke aphasia. Multimodal imaging (fMRI, DTI, EEG) delineates dynamic language network reorganization across recovery stages, guiding targeted NIBS strategies. In the acute phase, inhibitory stimulation modulates right-hemisphere hyperactivity; in the subacute phase, bilateral facilitation supports network rebalancing; and in the chronic phase, excitatory stimulation enhances left perilesional plasticity. This framework integrates stage-dependent imaging biomarkers with tailored neuromodulation to optimize individualized language recovery.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-07-30
Accepted 2025-10-25
Published 2025-11-20