



Abstract
Deep Brain Stimulation (DBS) is a well-established surgical therapy for advanced Parkinson's disease
(PD), effectively alleviating
motor symptoms and complications associated with long-term levodopa treatment. This review provides a
comprehensive synthesis of
current evidence, analyzing the efficacy of the two primary targets, the subthalamic nucleus (STN) and
the globus pallidus internus
(GPi), on both motor and non-motor symptoms. While STN-DBS allows significant medication reduction and
GPi-DBS may better manage
dyskinesias and axial symptoms, outcomes are highly dependent on careful patient selection. Key
prognostic factors include
preoperative levodopa responsiveness, disease duration, motor phenotype, and cognitive status. The
review also critically evaluates
technological advancements, such as adaptive closed-loop systems and novel targets, which aim to
personalize therapy and address
treatment-resistant symptoms. Ultimately, DBS represents a transformative intervention whose success
hinges on integrated clinical
decision-making and continued innovation.
Keywords: Parkinson's disease; deep brain stimulation; subthalamic nucleus; globus pallidus internus; prognostic factors.
Introduction
Parkinson's disease (PD) is the second most common neurodegenerative disorder after Alzheimer's disease, imposing a significant and growing burden on global health systems [1-3]. Its core pathological hallmark is the degeneration of dopaminergic neurons in the substantia nigra pars compacta, leading to dopamine depletion in the striatum and consequent dysfunction of the cortico-basal ganglia-thalamocortical loops [4-6]. Clinically, PD manifests cardinal motor symptoms including tremor at rest, bradykinesia, rigidity, and, as the disease evolves, postural instability and gait disturbances [7, 8]. The introduction of levodopa in the 1960s revolutionized PD treatment, providing remarkable symptomatic relief [9-11]. However, long-term levodopa therapy is inevitably complicated by the development of motor fluctuations (the "wearing-off" and "on-off" phenomena) and levodopa-induced dyskinesias (LID), which severely impair quality of life [10, 12, 13].
For patients with these advanced, medication-refractory complications, deep brain stimulation (DBS) has become a standard of care [14-16]. DBS involves the stereotactic implantation of electrodes into specific deep brain nuclei, connected to a subcutaneous implantable pulse generator that delivers continuous high-frequency electrical stimulation [17-19]. Since its widespread adoption in the late 1990s, DBS has demonstrated robust, long-term efficacy in ameliorating motor symptoms, reducing motor complications, and decreasing medication requirements [20, 21]. The two primary and most validated targets for PD are the subthalamic nucleus (STN) and the globus pallidus internus (GPi), each with a distinct profile of benefits and potential side effects [22, 23].
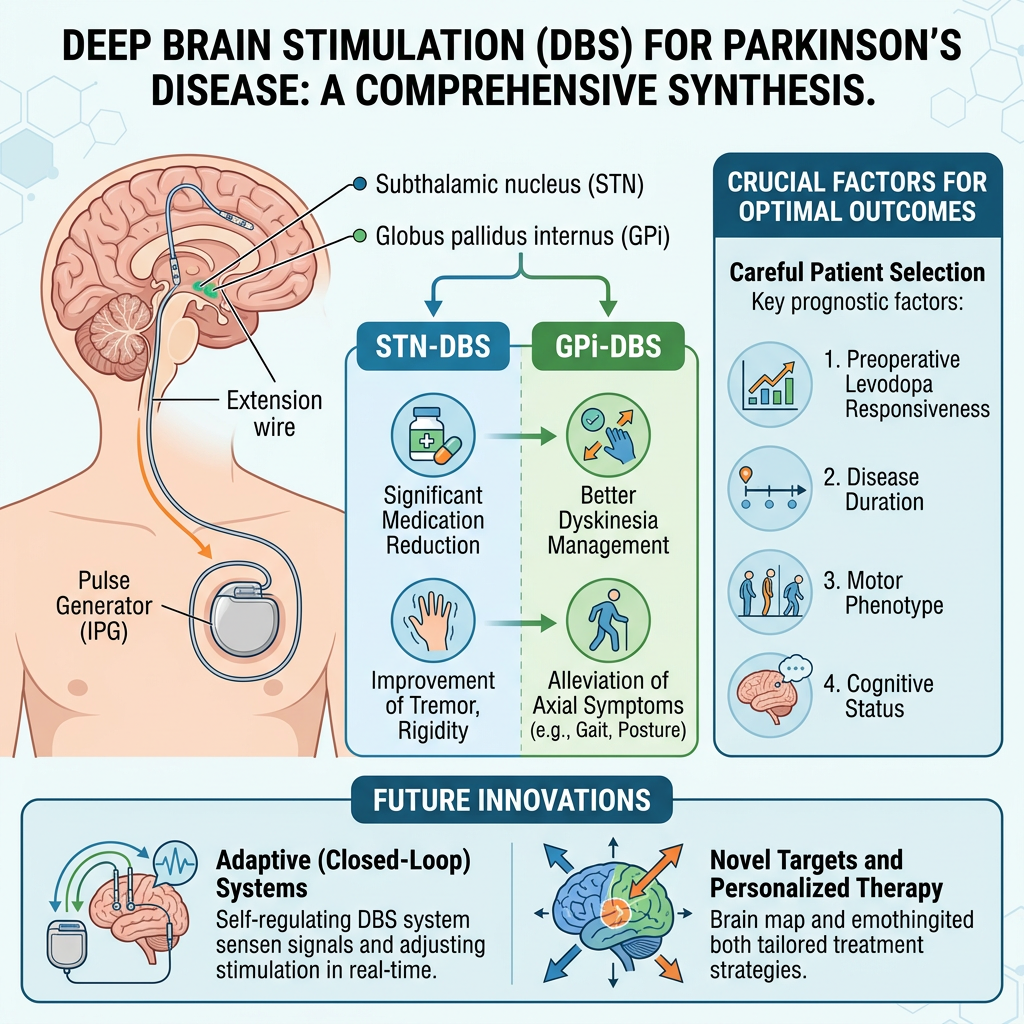
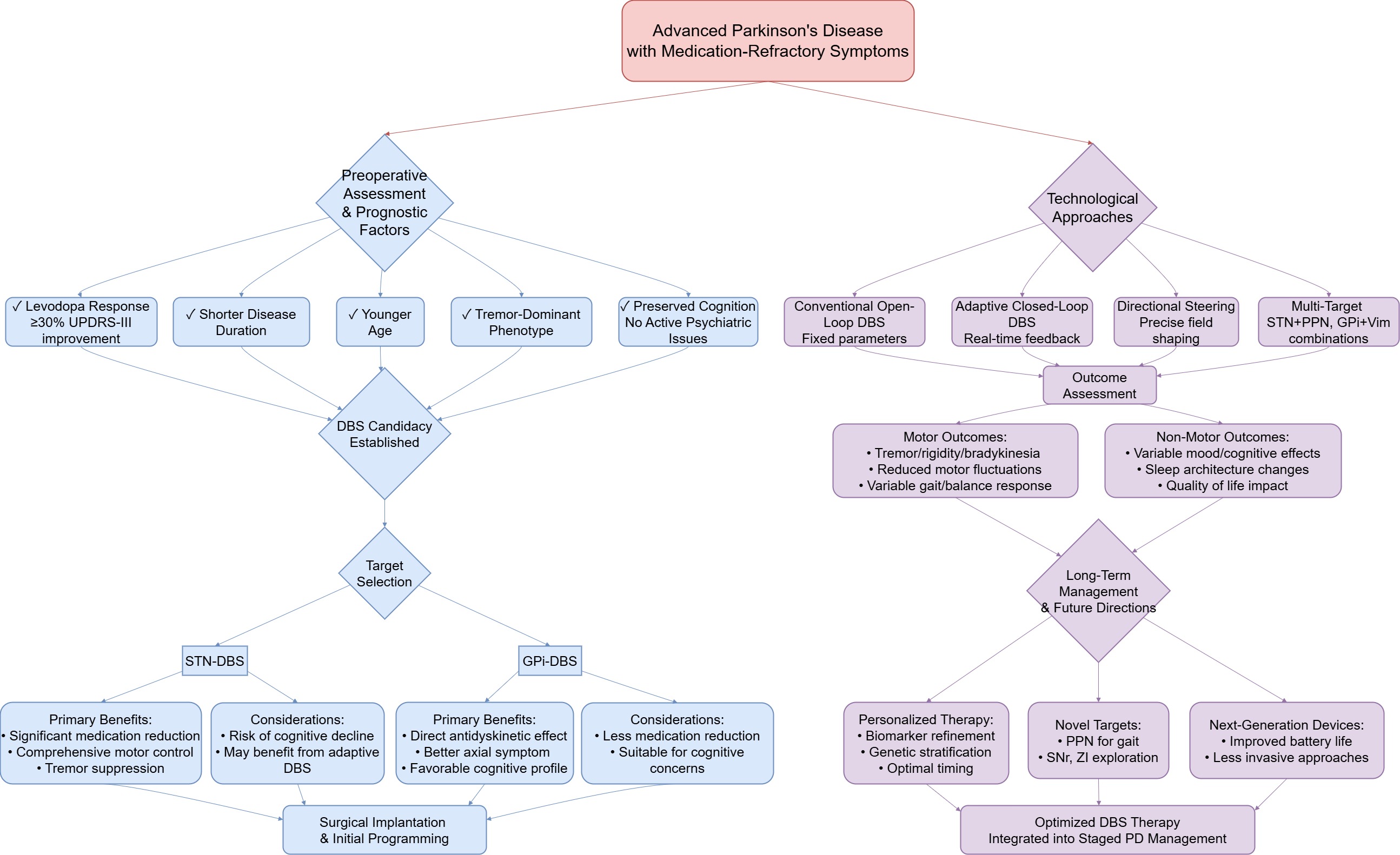
The objective of this review is to provide a comprehensive and systematic analysis of the current state of DBS for PD. It will synthesize evidence on the efficacy of DBS across the spectrum of motor and non-motor symptoms, delve into the critical patient and disease characteristics that predict surgical outcomes, and offer a critical evaluation of technological advancements and future research trajectories. By moving beyond a mere cataloging of effects to a nuanced discussion of mechanisms, predictors, and evolving paradigms, this review aims to consolidate knowledge for clinicians and researchers, and to identify key areas where further investigation is needed to optimize this powerful neuromodulation therapy (Figure 1).
Figure 1. Clinical decision pathway and technological evolution of deep brain stimulation (DBS) in Parkinson's disease (PD).
Efficacy of DBS on Motor Symptoms
The therapeutic impact of DBS on the major motor features of PD is well-documented and constitutes the primary rationale for its use [12, 24]. The magnitude of improvement, however, varies by symptoms and targets (Table 1).
To appreciate the differential effects of stimulating these two nuclei, a basic understanding of basal ganglia circuitry is essential. The basal ganglia are organized into parallel, functionally segregated loops that modulate cortical activity [4]. Within the motor loop, the striatum (putamen) receives cortical input and projects to the output nuclei as GPi and substantia nigra pars reticulata (SNr) via two main pathways: the direct and indirect pathways. The direct pathway, which facilitates movement, involves monosynaptic inhibitory projections from the striatum to the GPi/SNr. The indirect pathway, which suppresses unwanted movement, is a polysynaptic circuit involving the globus pallidus externus (GPe) and the STN [22].
The STN is a small, glutamatergic nucleus strategically positioned as a key driver of the indirect pathway. Excitatory output from the STN to the GPi/SNr serves to inhibit thalamocortical projections, thereby suppressing movement [36]. In PD, dopaminergic depletion in the striatum leads to overactivity of the STN, resulting in excessive excitatory drive to the GPi/SNr and pathological inhibition of the thalamus and cortex, which manifests as bradykinesia and rigidity [4]. In contrast, the GPi is the primary output nucleus of the basal ganglia, integrating inputs from both the direct and indirect pathways to send inhibitory signals to the thalamus [23]. In the parkinsonian state, GPi neurons exhibit abnormally high and burst-like firing rates, contributing to the same net inhibitory effect on thalamocortical circuits. Thus, while both nuclei become hyperactive in PD, the STN functions as a driving force within the indirect pathway, whereas the GPi serves as a final common output. This distinction as STN acts modulator of network drive and GPi as a regulator of final output provides a neurobiological rationale for the observed clinical differences: STN-DBS may achieve its marked levodopa-sparing effect by directly modulating a key node in the indirect pathway, while GPi-DBS might more directly control dyskinesias by normalizing the abnormal output patterns that generate these involuntary movements.
Table 1. Comparative overview of STN-DBS and GPi-DBS in Parkinson's disease.
| Aspect | STN-DBS | GPi-DBS |
|---|---|---|
| Primary Motor Benefits | Significant reduction in tremor, rigidity, bradykinesia; marked decrease in daily "off" time. | Comparable tremor control; strong direct antidyskinetic effect; potentially better for axial symptoms. |
| Levodopa Reduction | Often allows 30–50% reduction in dopaminergic medication. | Usually does not permit major medication reduction; controls dyskinesias directly. |
| Non-Motor Effects | May improve depression; risk of apathy, mild decline in verbal fluency/executive function; possible daytime sleepiness. | Generally neutral or slightly positive mood profile; minimal cognitive adverse effects. |
| Ideal Candidate Profile | Younger age, good levodopa response, tremor-dominant subtype, need for medication reduction. | Significant dyskinesias, axial symptoms, cognitive concerns, older patients. |
| Key Considerations | Requires careful neuropsychological screening; postoperative apathy management; battery life extended with adaptive systems. | Less medication flexibility; may be preferable in patients with mild cognitive impairment or psychiatric vulnerability. |
Abbreviations: DBS, deep brain stimulation; GPi, globus pallidus internus; STN, subthalamic nucleus.
Resting tremor, often the most recognizable sign of PD [6], is exquisitely responsive to DBS [15]. STN is considered the target of choice for comprehensive symptom control, including tremor [25, 26]. STN-DBS produces rapid and dramatic tremor suppression, with 70-90% of patients experiencing significant relief immediately after surgery [17, 27]. This effect is remarkably durable, with studies reporting sustained benefit in 60-70% of patients after more than five years [20, 21]. The mechanism is thought to involve the disruption of pathological oscillatory activity within the cerebello-thalamo-cortical circuit [28-30]. GPi-DBS also provides substantial tremor control, with reported efficacy rates of 60-80%, and some meta-analyses suggest comparable effects between STN and GPi for tremor suppression [23, 26]. For patients with severe, medication-refractory tremor as the dominant symptom, the ventral intermediate nucleus (Vim) of the thalamus can be used either alone or in combination with other targets (e.g., GPi plus Vim) to achieve superior tremor control, though it offers less benefit for other PD features like bradykinesia and rigidity [31-33].
Rigidity and BradykinesiaRigidity and bradykinesia are core symptoms that profoundly affect manual dexterity and movement initiation [34]. Both STN-DBS and GPi-DBS produce major improvements in these domains [15]. STN-DBS typically leads to a 40-60% reduction in limb rigidity scores on standardized scales like the UPDRS-III [22]. Bradykinesia, assessed through tasks like finger tapping, shows improvement with increased movement speed of 20-40% [17]. These effects are frequency-dependent, with stimulation above 130 Hz generally providing optimal results [35]. The underlying mechanism involves the modulation of the hyperdirect and indirect pathways, normalizing the excessive inhibitory output from the basal ganglia to thalamocortical projections [36, 37]. GPi-DBS demonstrates broadly similar efficacy for rigidity and bradykinesia, though its mechanism is centered on direct modulation of the output nucleus of the basal ganglia [38]. The choice between targets for these symptoms is often influenced by other factors, such as the need for medication reduction or the presence of dyskinesias [15].
Postural Instability and Gait DisordersAxial symptoms, including postural instability, freezing of gait (FOG), and festination, represent a major therapeutic challenge in advanced PD and are less predictably improved by DBS [39, 40]. In the short to medium term (1-2 years), STN-DBS can provide meaningful benefit, reducing FOG episodes by 30-50% and improving gait speed [39, 40]. However, its effect on postural reflexes is modest (20-30% improvement), and long-term studies indicate that the risk of falls often returns to baseline after five years, suggesting DBS does not halt the underlying neurodegenerative progression in brainstem locomotor centers [41]. GPi-DBS may offer a slight advantage over STN-DBS in maintaining postural stability, potentially due to differential effects on brainstem circuits [42, 43]. To address this critical unmet need, novel targets are being explored. Low-frequency stimulation (60-80 Hz) of the STN or dedicated stimulation of the pedunculopontine nucleus (PPN), a key node in the mesencephalic locomotor region, has shown promise in further improving gait and balance, particularly FOG [44, 45]. Innovative paradigms like variable-frequency stimulation, alternating between high and low frequencies, are under investigation to provide balanced improvement across all symptom domains [46, 47].
Motor ComplicationsOne of the most significant benefits of DBS is its ability to mitigate the long-term complications of levodopa therapy. DBS dramatically smooths out motor fluctuations. STN-DBS can reduce daily "off" time by approximately 50% and increase "on" time without troublesome dyskinesias by 3-4 hours per day [15, 48]. This is achieved through a combination of direct symptom control and the subsequent ability to significantly reduce dopaminergic medication (often by 30-50%) [49, 50]. GPi-DBS also effectively increases "on" time, even without substantial medication reduction, by directly modulating the basal ganglia output [23].
Regarding levodopa-induced dyskinesias (LID), the two targets act through different mechanisms. GPi-DBS has a direct anti-dyskinetic effect, often reducing LID severity by over 50% shortly after activation, likely by suppressing the abnormal pallidal output driving dyskinetic movements [23]. STN-DBS primarily reduces LID indirectly by enabling major medication reduction, though some studies suggest a direct suppressive effect, especially when stimulating dorsal regions of the STN [51].
Combined Pharmacotherapy and DBSWhile DBS markedly reduces motor fluctuations and levodopa-induced dyskinesias, it does not completely obviate the need for pharmacotherapy in most patients. Postoperative medication management is a nuanced process that must be individualized based on the stimulation target and the patient's clinical response. For patients undergoing STN-DBS, the significant levodopa-sparing effect (typically 30-50% reduction) is a key advantage, allowing for substantial dose reduction of dopaminergic drugs to minimize side effects such as impulse control disorders and dopaminergic psychosis [49, 50]. However, complete withdrawal is rarely advisable, as a baseline level of dopaminergic tone may be necessary to support non-motor functions and mood, and abrupt cessation can precipitate apathy or depression. In contrast, patients with GPi-DBS often require maintenance of their preoperative medication levels to achieve optimal motor benefit, as this target has less direct impact on medication requirements [23, 38].
Beyond dopaminergic drugs, the role of adjunctive medications remains important. For axial symptoms like freezing of gait that may persist or emerge despite optimal DBS and levodopa adjustment, agents such as MAO-B inhibitors (e.g., rasagiline) or amantadine can provide additional benefit [40, 47]. Furthermore, the management of non-motor symptoms, including depression, anxiety, and sleep disturbances, frequently necessitates the use of antidepressants, anxiolytics, or hypnotics in conjunction with DBS. The interaction between stimulation parameters and drug pharmacokinetics/pharmacodynamics is an area of ongoing investigation, with emerging evidence suggesting that closed-loop DBS systems may eventually enable real-time, automated coordination with medication cycles to further smooth out symptom fluctuations. Thus, DBS should be conceptualized not as a replacement for pharmacotherapy but as a powerful adjunct that, when optimally combined with medications, offers the best chance for comprehensive symptom control in advanced PD.
Impact of DBS on Non-Motor Symptoms
The effects of DBS extend beyond the motor system, influencing neuropsychiatric, cognitive, and sleep domains. These non-motor outcomes are complex, variable, and critically important for overall patient well-being [52].
Neuropsychiatric SymptomsDBS exerts nuanced effects on mood and behavior, heavily influenced by the stimulation target. STN-DBS can lead to improvements in depressive symptoms in many patients, potentially linked to the modulation of limbic circuits adjacent to the motor STN [53]. However, in 5-10% of cases, it can induce or exacerbate depression, possibly via interference with serotonergic projections [54]. GPi-DBS generally has a more neutral or slightly positive profile regarding mood [54]. Anxiety symptoms often improve with stimulation of either target, correlating with both direct neuromodulation and the secondary psychological benefit of improved motor function [53, 55]. A significant concern is the development of apathy, which can occur post-STN-DBS, potentially related to rapid dopamine agonist withdrawal or direct effects on motivational circuits [56]. Careful postoperative medication management and parameter adjustment are essential to mitigate these psychiatric risks [57].
Cognitive FunctionThe cognitive consequences of DBS are a critical consideration in patient selection and postoperative management [58]. STN-DBS is associated with mild but measurable declines in specific cognitive domains, particularly verbal fluency and executive functions (e.g., set-shifting, response inhibition), with meta-analyses confirming small-to-moderate effect sizes [54, 59]. These changes are more pronounced with bilateral stimulation and are thought to arise from multiple mechanisms.
A growing body of evidence implicates current spread from the motor territory of the STN to its adjacent associative and limbic subdivisions, which are involved in cognitive and emotional processing [60]. The STN is anatomically and functionally divided into three territories: the dorsolateral motor portion, the ventromedial associative portion, and the medial limbic portion. High-frequency stimulation optimized for motor symptom control may inadvertently modulate neurons or passing fibers within these non-motor territories, disrupting cognitive networks [60]. This is supported by diffusion tensor imaging studies showing that stimulation volumes intersecting with hyperdirect pathways from prefrontal cortex correlate with executive function declines.
Recent advances in resting-state functional MRI have provided deeper insights into the network-level effects of DBS. A pivotal study by Luo et al. demonstrated that cognitive decline following STN-DBS is associated with a widespread reduction in functional connectivity within cognitive-related brain networks, particularly the default mode network (DMN) and frontoparietal executive network [61]. Using preoperative and postoperative resting-state fMRI in patients with Parkinson's disease, the authors showed that individuals who exhibited significant cognitive deterioration at 12 months post-surgery demonstrated greater stimulation-induced decreases in connectivity between the posterior cingulate cortex (a key DMN hub) and lateral prefrontal regions. Furthermore, the degree of connectivity reduction correlated with the magnitude of decline on neuropsychological tests of attention and executive function. This network-level mechanism suggests that DBS exerts its cognitive effects not merely through local modulation of the STN, but through broader disruption of large-scale brain networks that support cognitive processing.
Patient-specific factors significantly modulate this risk. Individuals with pre-existing mild cognitive impairment (MCI) are particularly vulnerable, likely due to reduced cognitive reserve and already-compromised network integrity [62, 63]. Longitudinal studies indicate that while DBS itself does not increase the rate of conversion to dementia compared to the natural history of PD, patients with MCI at the time of surgery have a higher probability of progressing to dementia than non-operated patients with similar baseline cognitive status [62]. This underscores the necessity of rigorous preoperative neuropsychological screening to identify at-risk individuals.
In contrast, GPi-DBS appears to have a more favorable cognitive profile, with meta-analyses showing minimal negative impact and possible improvement in some executive tasks [52, 58]. This difference may reflect the anatomical position of the GPi as a downstream output nucleus, where stimulation effects are more confined to motor circuits with less spread to associative networks. Alternatively, the absence of a medication-sparing effect with GPi-DBS means that patients maintain their dopaminergic therapy, which may provide ongoing cognitive support, as dopamine is known to modulate prefrontal cortical function.
Sleep and AlertnessDBS can positively influence sleep architecture, primarily by alleviating nocturnal akinesia, pain, and tremor, thereby improving sleep continuity and increasing deep sleep (N3 stage) duration [64, 65]. STN-DBS has been shown to reduce the severity of restless legs syndrome (RLS) in PD patients [66]. Its effect on REM sleep behavior disorder (RBD) is less clear, with studies reporting partial improvement in dream-enactment behaviors but persistence of abnormal muscle activity [67, 68]. A notable side effect is the potential for STN-DBS to induce or exacerbate daytime sleepiness, possibly via inhibition of wake-promoting hypothalamic nuclei [69, 70]. GPi-DBS's effects on specific sleep disorders like RLS and RBD are less studied but may follow a similar pattern of benefit driven by overall symptom improvement [64].
Prognostic Factors and Patient Selection
The success of DBS is not uniform; it is highly contingent on appropriate patient selection. Identifying robust predictors of outcome is paramount for maximizing benefit and minimizing risk [71, 72].
Levodopa ResponsivenessA positive response to a preoperative levodopa challenge test is the strongest independent predictor of favorable motor outcome after DBS [71, 72]. An improvement of ≥30% in the UPDRS-III motor score during the "on" medication state is widely used as a key inclusion criterion [15, 16, 22]. This response indicates the presence of a functional dopaminergic system and suggests that the patient's disability is primarily due to dopaminergic deficiency rather than unresponsive non-dopaminergic pathology (e.g., widespread Lewy body disease affecting cholinergic or noradrenergic systems) [72]. While predictive of excellent short- and medium-term outcomes, the predictive value of the levodopa test may diminish for very long-term prognosis (>5 years) as non-dopaminergic symptoms emerge [73].
Disease Duration and Age at SurgeryShorter disease duration is consistently associated with superior and more durable motor outcomes after DBS [71]. Patients with advanced disease and long duration (>10 years) often have significant involvement of non-dopaminergic systems (e.g., pedunculopontine nucleus, locus coeruleus), leading to axial symptoms, cognitive impairment, and autonomic dysfunction that are less amenable to DBS [74, 75]. Consequently, there is a growing trend toward considering DBS at an earlier stage, once troublesome motor complications emerge, to preserve quality of life and possibly achieve better long-term functional outcomes [76].
Younger age at surgery is another favorable prognostic factor, linked to greater neural plasticity, better tolerance of stimulation, a lower burden of comorbidities, and a longer horizon to benefit from the therapy [75, 76]. Older patients (>70-75 years) may have reduced surgical and cognitive reserve, higher rates of brain atrophy (increasing surgical risk), and more vascular comorbidities (e.g., leukoaraiosis), which can limit DBS efficacy and increase perioperative complication rates [77, 78].
Motor PhenotypeThe predominant preoperative motor phenotype influences DBS outcome [72]. The "tremor-dominant" subtype is associated with excellent and sustained response to both STN and GPi DBS [79]. In contrast, patients with the "postural instability/gait difficulty" (PIGD) phenotype typically experience less robust and less durable improvement, particularly for their axial symptoms [80]. This subtype is also linked to faster disease progression and higher prevalence of cognitive decline [81]. These differences suggest underlying variations in the topographic spread of pathology and neurochemical deficits among PD subtypes [80, 81].
An emerging conceptual framework with potential relevance to DBS outcomes is the classification of PD into "brain-first" and "body-first" subtypes based on the initial site of α-synuclein pathology accumulation. Although direct evidence examining DBS outcomes stratified by these subtypes is currently limited, theoretical considerations suggest possible differences in treatment response. Patients with the body-first subtype, characterized by earlier and more RBD and greater brainstem pathology [68], may be predisposed to persistent axial symptoms post-DBS due to greater involvement of non-dopaminergic brainstem locomotor centers such as the pedunculopontine nucleus [39, 44]. Conversely, brain-first patients, who have a higher propensity for cognitive decline and neuropsychiatric features, may face increased risks of postoperative cognitive deterioration if stimulation spreads to non-motor territories [61, 62]. This framework highlights the importance of assessing non-motor features, particularly RBD and cognitive status, when counseling patients about expected outcomes, and prospective studies incorporating these variables are needed to formally test whether this classification can refine patient selection.
Cognitive and Psychiatric BaselinePreoperative cognitive status is a critical determinant of postoperative outcome and risk [59]. Significant cognitive impairment or dementia is a contraindication to DBS, as surgery can worsen cognition and does not improve functional independence in this population [52]. The presence of MCI necessitates careful counseling, as it increases the risk of further decline [59, 63]. Similarly, active, untreated major depression, anxiety, or psychosis are contraindications, as DBS can exacerbate these conditions [15, 16, 22]. Stable, well-managed psychiatric disorders require close multidisciplinary management perioperatively [52, 58].
Technological Developments and Future Directions
The field of DBS is rapidly evolving beyond traditional, constant-parameter ("open-loop") stimulation [82, 83].
Adaptive or Closed-Loop DBS (aDBS)aDBS represents a paradigm shift. Instead of delivering fixed stimulation, aDBS systems use implanted sensors to record local field potential (LFP) [84, 85], such as beta-band oscillations from the STN, which correlate with motor symptom severity [86]. The stimulator then automatically adjusts its output in real-time based on this neural feedback [87]. Early clinical studies show that aDBS can provide equivalent or superior symptom control compared to conventional DBS while significantly reducing total stimulation energy delivery, potentially extending battery life and reducing stimulation-induced side effects [88, 89].
Directional Steering and Current FractionationModern DBS leads with multiple segmented contacts allow for "directional" steering of the electrical field [90]. This enables clinicians to shape the volume of tissue activated, more precisely targeting the therapeutic zone while avoiding stimulation of adjacent structures responsible for side effects (e.g., corticospinal tract causing muscle contractions, medial limbic STN affecting mood) [91]. This technology enhances the therapeutic window and allows for more personalized programming [92].
Novel Targets and Multi-Target StimulationTo address therapy-resistant symptoms, new targets are being investigated. As mentioned, PPN stimulation for gait and balance is a primary focus [44, 93]. The substantia nigra pars reticulata (SNr) and the zona incerta are also being explored [31]. Furthermore, the simultaneous use of two targets (e.g., STN plus PPN, GPi plus Vim) in a single patient via a single or dual generator system is being studied to provide a broader spectrum of symptom control [32].
Future Research and Critical PerspectivesDespite its established efficacy, several critical questions remain. Long-term (>10 year) outcomes data, especially regarding the evolution of non-motor symptoms and quality of life, are still maturing [21]. The optimal timing of DBS intervention is an area of active debate and ongoing clinical trials (e.g., the EARLYSTIM study extension) in balancing early benefits against surgical risks and natural disease progression [71, 76]. Further refinement of patient selection biomarkers, beyond clinical assessments, using neuroimaging, genetics, and electrophysiology, is needed [72]. Finally, the cost-effectiveness and accessibility of DBS, along with the development of even less invasive neuromodulation techniques, will be crucial for broadening its global impact [14].
Conclusion
Deep Brain Stimulation has irrevocably changed the treatment landscape for advanced PD. It is a highly effective therapy for ameliorating levodopa-responsive motor symptoms and reducing debilitating motor complications, with proven long-term benefits. The choice between STN and GPi involves a nuanced trade-off, considering desired medication reduction, the profile of motor symptoms (especially axial features), and the patient's cognitive and psychiatric status. The non-motor effects of DBS are multifaceted and necessitate comprehensive preoperative assessment and postoperative management. The robustness of the outcome is heavily dependent on careful patient selection, with preoperative levodopa responsiveness, disease duration, phenotype, and cognitive/psychiatric health serving as key prognosticators.
The future of DBS lies in personalization and technological sophistication. Adaptive closed-loop systems, directional leads, and exploration of novel targets promise to enhance efficacy, reduce side effects, and tackle currently unmet needs like gait freezing. As research continues to refine patient selection criteria and stimulation strategies, DBS will solidify its role not merely as a last-resort intervention, but as an integral component of a personalized, staged therapeutic strategy for PD, aimed at preserving function and quality of life throughout the course of the disease.
Abbreviations
PD, Parkinson’s disease; DBS, deep brain stimulation; GPi, glo-bus pallidus internus; STN, subthalamic nucleus; LID, levodo-pa-induced dyskinesias; SNr, substantia nigra pars reticulata; GPe, globus pallidus externus; FOG, freezing of gait.
Declarations
Acknowledgements
None.
Author Contributions
SW designed the study, collected data, analyzed data, illustrat-ed figures, drafted the manuscript, and revised the manuscript. XL, RW, and RM collected data, analyzed data, and revised the manuscript. AY and FM designed the study, collected data, an-alyzed data, and revised the manuscript. JZ is the team leader who designed the study, collected data, analyzed data, and re-vised the manuscript. All authors have read and approved the final manuscript.
Acknowledgements
None.
Funding information
None.
Ethics Approval and Consent to Participate
N/A.
Competing Interests
The authors declare that they have no conflict of interest.
Data availability
The data that support the findings of this study are included in the article/supplementary material.
References
[2] Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021;397(10291):2284–303.
[7] Hayes MT. Parkinson's Disease and Parkinsonism. Am J Med. 2019;132(7):802–7.
[8] Tanner CM, Ostrem JL. Parkinson's Disease. N Engl J Med. 2024;391(5):442–52.
[34] Reich SG, Savitt JM. Parkinson's Disease. Med Clin North Am. 2019;103(2):337–50.
[37] McGregor MM, Nelson AB. Circuit Mechanisms of Parkinson's Disease. Neuron. 2019;101(6):1042–56.
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Clinical decision pathway and technological evolution of deep brain stimulation (DBS) in Parkinson's disease (PD). This schematic summarizes the integrated process from patient selection to long-term management. Patient Selection Criteria: highlights essential preoperative predictors of favorable outcome, including robust levodopa responsiveness, shorter disease duration, and younger age. Target Selection: contrasts the principal surgical targets as subthalamic nucleus (STN) and globus pallidus internus (GPi) based on their distinct benefit-risk profiles. Technological Approaches: outlines available stimulation strategies, from conventional open-loop to adaptive closed-loop and directional steering systems. Outcome Assessment: encompasses both motor and non-motor domains, reflecting the multidimensional impact of DBS. Future Directions: points toward personalized therapy, novel targets, and next-generation devices that aim to broaden efficacy and accessibility. Abbreviations: DBS = deep brain stimulation; STN = subthalamic nucleus; GPi = globus pallidus internus.
[2] Bloem BR, Okun MS, Klein C. Parkinson's disease. Lancet. 2021;397(10291):2284–303.
[7] Hayes MT. Parkinson's Disease and Parkinsonism. Am J Med. 2019;132(7):802–7.
[8] Tanner CM, Ostrem JL. Parkinson's Disease. N Engl J Med. 2024;391(5):442–52.
[34] Reich SG, Savitt JM. Parkinson's Disease. Med Clin North Am. 2019;103(2):337–50.
[37] McGregor MM, Nelson AB. Circuit Mechanisms of Parkinson's Disease. Neuron. 2019;101(6):1042–56.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2026-01-08
Accepted 2026-03-10
Published 2026-03-30