



Abstract
Objective: To explore the efficacy of middle meningeal artery embolization (MMAE) in the treatment of chronic subdural hematoma (CSDH).
Methods: We retrospectively analyzed clinical data of 3 patients (with 4-sided hematomas) diagnosed with CSDH who were admitted to the Department of Neurosurgery, General Hospital of Ningxia Medical University in December 2021. Two patients underwent MMAE (one with bilateral MMA embolization), and one patient received MMAE combined with subdural burr hole drainage. All patients were embolized using Onyx glue. Clinical efficacy was evaluated using the modified Rankin Scale (mRS), with a ≥1-point decrease post-treatment defined as symptom improvement. Hematoma absorption was assessed via imaging.
Results: Successful superselective catheterization of the middle meningeal artery (MMA) was achieved in all 3 patients (4-sided hematomas), with complete occlusion of the frontoparietal trunk of the MMA and its main branches. No procedure-related complications occurred. During a 2–4 month follow-up, all patients showed clinical improvement (mRS decreased by 1–2 points). Imaging confirmed complete absorption of all 4-sided hematomas, resolution of clinical symptoms, and no recurrence.
Conclusion: MMAE is a safe, effective, and promising treatment for CSDH.
Keywords: MMAE, CSDH, mRS, Case Series.
Introduction
Chronic subdural hematoma (CSDH) is a common neurosur-gical condition, predominantly affecting elderly patients, and is associated with significant morbidity and mortality [1-3]. Current treatment modalities include conservative manage-ment, burr hole drainage, and hematoma evacuation [4]. Phar-macological options for CSDH primarily consist of steroids, platelet-activating factor antagonists, and statins [5]. However, conservative treatment success rates vary widely, with failure rates requiring surgical intervention ranging from 15% to 90% [4], and non-surgical approaches are only effective in select pa-tient subgroups [6-10]. Thus, surgical evacuation remains the mainstay for most CSDH cases [11]. Nevertheless, 5%–30% of surgical cases experience hematoma recurrence [12-17], partly because conventional surgery does not address the underlying pathophysiological mechanisms of CSDH formation [18-20].In recent years, middle meningeal artery embolization (MMAE) has emerged as a minimally invasive approach to target the vascular supply of CSDH, aiming to improve treatment out-comes [21]. This study evaluates the efficacy of MMAE in treating CSDH through a case series and literature review.
Materials and Methods
Clinical DataThree patients with CSDH were included: 2 males (1 with bilat-eral hematomas) and 1 female, aged 58–59 years (mean 58.3 years). All had a history of head trauma, with disease duration ranging from 23 to 60 days (mean 37.67 days) (Table 1).
Table 1. Clinical details of the three patients.
| Age (years) | Gender | Time from Onset (days) | Symptoms | Hematoma Location | Comorbidities | Surgical Method | Follow-up (months) |
|---|---|---|---|---|---|---|---|
| 59 | Male | 23 | Headache | Left frontal, parietal, temporal, occipital lobes | None | MMAE | 4 |
| 59 | Male | 30 | Headache | Bilateral frontal and temporal lobes | Hypertension (1 year) | MMAE | 2 |
| 58 | Female | 60 | Headache, left limb weakness | Right frontal and temporal lobes | None | MMAE + Burr hole drainage | 2 |
All patients were diagnosed with CSDH via preoperative cranial CT. One patient had bilateral hematomas, and 2 had unilateral hematomas. Hematoma types included 2 cases (3 sides) of isodense hematomas and 1 case (1 side) of mixed-type hema-tomas.
Treatment MethodPatients were placed in the supine position, with routine dis-infection and draping. The right femoral artery was punctured using the Seldinger technique, and a 6F arterial sheath was inserted. Cerebral angiography was performed, followed by systemic heparinization. Under fluoroscopic guidance, a 6F guiding catheter was advanced into the affected external ca-rotid artery using a 150 cm guidewire. A microcatheter was then navigated into the external carotid artery → maxillary artery → MMA under microguidewire guidance. After injecting DMSO as a solvent, 0.5 mL of Onyx glue was administered to embolize the affected MMA. The procedure was completed by withdrawing the microcatheter and guiding catheter.
Postoperative ManagementAll patients received postoperative fluid replacement. D-dimer levels were monitored on postoperative day 2:
- If D-dimer levels were not significantly elevated, patients were allowed early ambulation for rehabilitation.
- If D-dimer was elevated, lower extremity Doppler ultrasound was performed; ambulation was permitted if no deep vein thrombosis was detected.
Two patients underwent standalone MMAE with normal postoperative D-dimer levels and ambulated on postoperative day 1.
One patient (MMAE + burr hole drainage) had elevated D-dimer but no deep vein thrombosis; the surgical drain was removed at 30 hours, and ambulation was initiated thereafter.
Follow-upPatients were followed up via outpatient visits and telephone calls for 2–5 months. Neurological function was assessed using the mRS:
- 0: Asymptomatic
- 1: Symptomatic but no disability; able to perform all daily activities
- 2: Mild disability; independent in self-care but unable to resume previous activities
- 3: Moderate disability; walks unassisted but requires help with daily activities
- 4: Severe disability; unable to walk or self-care without assistance
- 5: Bedridden, incontinent, requiring long-term care
- 6: Death
Results
All 3 patients (4-sided hematomas) achieved successful superselective MMA catheterization, with complete occlusion of the frontoparietal trunk of the MMA and its main branches. No procedure-related complications occurred. During follow-up (2–5 months):
- All patients showed clinical improvement: 2 patients had mRS scores decrease from 2 to 0, and 1 patient improved from 3 to 0.
- Imaging confirmed complete absorption of all 4-sided hematomas, resolution of symptoms, and no recurrence (Figure 1–Figure 3).
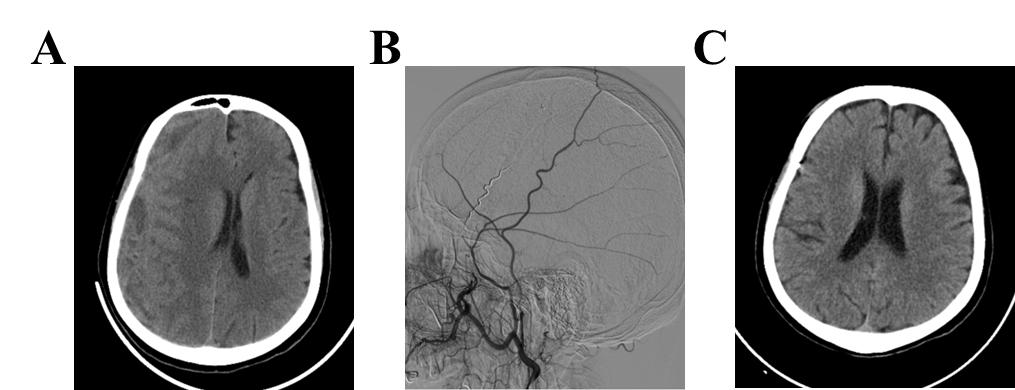
Figure 1. Preoperative CT showing left frontal, parietal, temporal, and occipital CSDH (A); left MMA embolization (B); 4-month follow-up CT showing complete hematoma absorption (C).
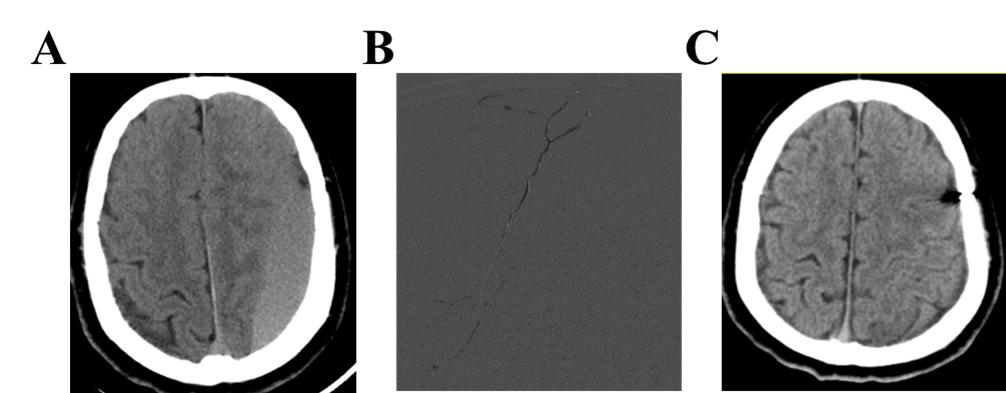
Figure 2. Preoperative CT showing bilateral frontal and temporal CSDH (A); bilateral MMA embolization (B); 2-month follow-up CT showing complete hematoma absorption (C).
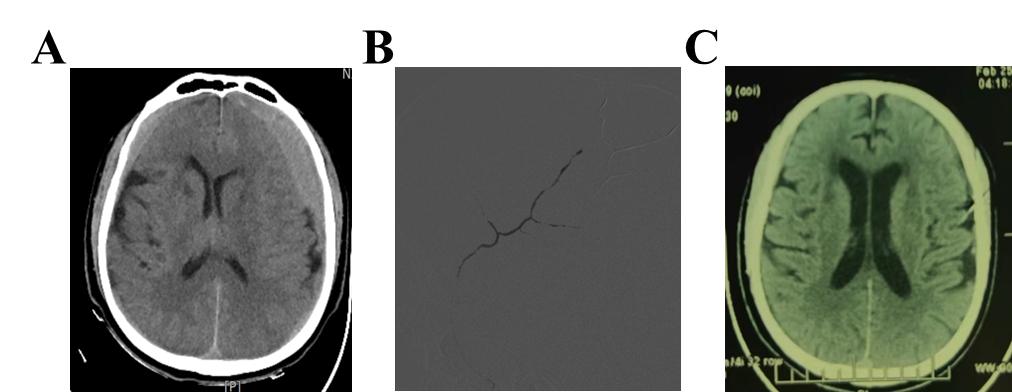
Figure 3. Preoperative CT showing right frontal and temporal CSDH (A); right MMA embolization (B); 2-month follow-up CT showing complete hematoma absorption (C).
Discussion
CSDH incidence is rising annually [22]. With population aging and increased use of anticoagulants/antiplatelets, the U.S. is projected to see >60,000 new cases yearly by 2030, making CSDH the most common adult neurosurgical diagnosis [1].The pathophysiology of CSDH involves complex processes. Historically attributed to traumatic bridging vein rupture [23, 24], inflammation is now recognized as a key driver [25, 26], explaining CSDH development in trauma-negative patients or those with delayed onset. Inflammation, membrane formation, angiogenesis, and fibrinolysis synergistically promote hemato-ma expansion [25]. Conventional surgery relieves mass effect but does not address these mechanisms, leading to recurrence [11, 21]. MMAE targets the vascular supply of CSDH, overcom-ing this limitation [21].
MMAE is applicable to all CSDH types, complementing drug therapy and burr hole drainage. It is particularly valuable for patients on long-term antiplatelets/anticoagulants, or with thrombocytopenia/coagulation disorders, except those with severe contrast allergies or renal insufficiency. Studies support MMAE’s efficacy: Fiorella et al. reported lower treatment failure rates with MMAE vs. standard therapy [27]; multicenter studies highlight its safety as a minimally invasive alternative [28-30].
In our series, 2 patients underwent MMAE (1 bilateral), and 1 received MMAE + burr hole drainage, with complete hemato-ma resolution and symptom improvement. MMAE works by occluding the MMA (a key blood supply to CSDH capsules) with Onyx glue, cutting off hematoma perfusion and prevent-ing recurrence. Compared to conventional surgery, it reduces infection, rebleeding, and brain tissue damage, enabling faster recovery—critical for elderly patients to minimize bedridden complications.
Limitations include the small sample size (3 patients, 4-sided hematomas) and short follow-up (2–4 months), which restrict generalizability and long-term efficacy assessment. Future multicenter, large-cohort studies with extended follow-up are needed to validate MMAE’s safety and optimize protocols.
Conclusion
MMAE or MMAE combined with burr hole drainage achieved successful occlusion of the MMA, complete hematoma absorption, symptom resolution, and no recurrence in 3 CSDH patients. Supported by literature, MMAE blocks hematoma blood supply, addressing limitations of traditional treatments, and is a safe, effective CSDH therapy. Further research with larger cohorts and longer follow-up is warranted to confirm its broader applicability and long-term outcomes.
Abbreviations
MMAE: Middle Meningeal Artery Embolization; CSDH: Chronic Subdural Hematoma; MMA: Middle Meningeal Artery; mRS: modified Rankin Scale; DMSO: Dimethyl Sulfoxide.
Declarations
Author Contributions
Dejun Huang and Xianhao Huo conceived the study. Xingguo Xu and Cunxin Zhu collected data, drafted the manuscript, and conducted literature reviews. Zhenxing Yang and Ji Yin revised imaging data. All authors contributed to discussions and final manuscript revisions.
Acknowledgment
Not applicable.
Funding Information
None.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Ningxia Medical University General Hospital (No. XJS2021120).
Competing Interests
The authors declare no competing interests.
Data Availability
The raw data supporting this study are available from the corresponding authors upon reasonable request.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Preoperative CT showing left frontal, parietal, temporal, and occipital CSDH (A); left MMA embolization (B); 4-month follow-up CT showing complete hematoma absorption (C).
Figure 2. Preoperative CT showing bilateral frontal and temporal CSDH (A); bilateral MMA embolization (B); 2-month follow-up CT showing complete hematoma absorption (C).
Figure 3. Preoperative CT showing right frontal and temporal CSDH (A); right MMA embolization (B); 2-month follow-up CT showing complete hematoma absorption (C).
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-09-07
Accepted 2025-09-11
Published 2025-11-15